

Evaluating a Model to Predict Primary Care Physician-Defined Complexity in a Large Academic Primary Care Practice-Based Research Network
- PMID: 26048275
- PMCID: PMC4636571
- DOI: 10.1007/s11606-015-3357-8
Evaluating a Model to Predict Primary Care Physician-Defined Complexity in a Large Academic Primary Care Practice-Based Research Network
Abstract
Background: Improving the ability to risk-stratify patients is critical for efficiently allocating resources within healthcare systems.
Objective: The purpose of this study was to evaluate a physician-defined complexity prediction model against outpatient Charlson score (OCS) and a commercial risk predictor (CRP).
Design: Using a cohort in which primary care physicians reviewed 4302 of their adult patients, we developed a predictive model for estimated physician-defined complexity (ePDC) and categorized our population using ePDC, OCS and CRP.
Participants: 143,372 primary care patients in a practice-based research network participated in the study.
Main measures: For all patients categorized as complex in 2007 by one or more risk-stratification method, we calculated the percentage of total person time from 2008-2011 for which eligible cancer screening was incomplete, HbA1c was ≥ 9 %, and LDL was ≥ 130 mg/dl (in patients with cardiovascular disease). We also calculated the number of emergency department (ED) visits and hospital admissions per person year (ppy).
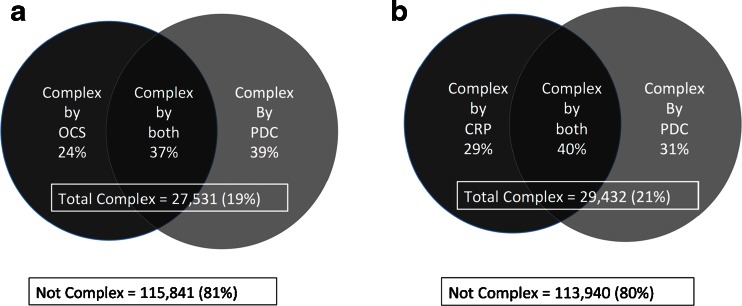
Key results: There was modest agreement among individuals classified as complex using ePDC compared with OCS (36.7 %) and CRP (39.6 %). Over 4 follow-up years, eligible ePDC-complex patients had higher proportions (p < 0.001) of time with: incomplete cervical (17.8 % vs. 13.3 % for OCS; 19.4 % vs. 11.2 % for CRP), breast (21.4 % vs. 14.9 % for OCS; 22.7 % vs. 15.0 % for CRP), and colon (25.9 % vs. 18.7 % for OCS; 27.0 % vs. 18.2 % for CRP) cancer screening; HbA1c ≥ 9 % (15.6 % vs. 8.1 % for OCS; 15.9 % vs. 6.9 % for CRP); and LDL ≥ 130 mg/dl (12.4 % vs. 7.9 % for OCS; 11.8 % vs 9.0 % for CRP). ePDC-complex patients had higher rates (p < 0.003) of: ED visits (0.21 vs. 0.11 ppy for OCS; 0.17 vs. 0.15 ppy for CRP), and admissions in patients 45-64 and ≥ 65 years old (0.11 vs. 0.10 ppy AND 0.24 vs. 0.21 ppy for OCS).
Conclusion: Our measure for estimated physician-defined complexity compared favorably to commonly used risk-prediction approaches in identifying future suboptimal quality and utilization outcomes.
Figures
Comment in
-
The Complexity of Complex Patients.J Gen Intern Med. 2015 Dec;30(12):1724-5. doi: 10.1007/s11606-015-3472-6. J Gen Intern Med. 2015. PMID: 26259761 Free PMC article. No abstract available.
References
-
- AHRQ, Agency for Healthcare Research and Quality. Closing the quality gap: A critical analysis of quality improvement strategies. 2007;7.
-
- Atlanticare Special Care Center. Special care center. http://www.atlanticare.org/index.php/special-care-center. Accessed April 1, 2015.
-
- Bell J, Mancuso D, and Krupski TE. A. A randomized controlled trial of king county partners' rethinking care intervention: Health and social outcomes up to two years post-randomization. 2012.
-
- Cohen SB, Yu W. The concentration and persistence in the level of health expenditures over time: Estimated the U.S. population, 2008–2009. Med Expenditure Panel Surv. 2012;Statistical Brief #354.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
