

Competing Risk Analysis of Neurologic versus Nonneurologic Death in Patients Undergoing Radiosurgical Salvage After Whole-Brain Radiation Therapy Failure: Who Actually Dies of Their Brain Metastases?
- PMID: 26050609
- PMCID: PMC4544707
- DOI: 10.1016/j.ijrobp.2015.04.032
Competing Risk Analysis of Neurologic versus Nonneurologic Death in Patients Undergoing Radiosurgical Salvage After Whole-Brain Radiation Therapy Failure: Who Actually Dies of Their Brain Metastases?
Abstract
Purpose: To estimate the hazard for neurologic (central nervous system, CNS) and nonneurologic (non-CNS) death associated with patient, treatment, and systemic disease status in patients receiving stereotactic radiosurgery after whole-brain radiation therapy (WBRT) failure, using a competing risk model.
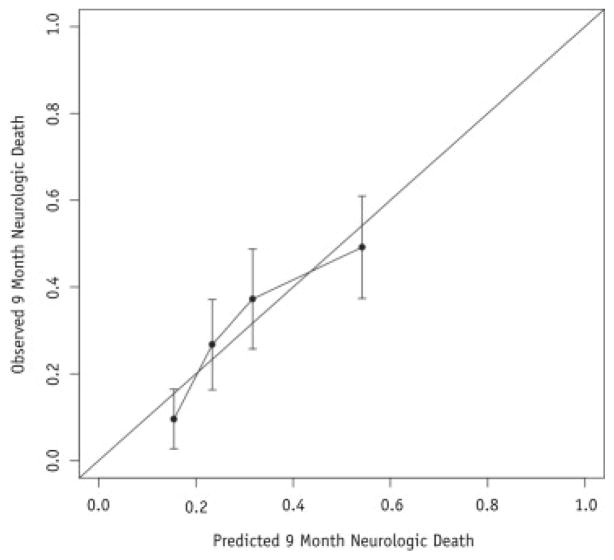
Patients and methods: Of 757 patients, 293 experienced recurrence or new metastasis following WBRT. Univariate Cox proportional hazards regression identified covariates for consideration in the multivariate model. Competing risks multivariable regression was performed to estimate the adjusted hazard ratio (aHR) and 95% confidence interval (CI) for both CNS and non-CNS death after adjusting for patient, disease, and treatment factors. The resultant model was converted into an online calculator for ease of clinical use.
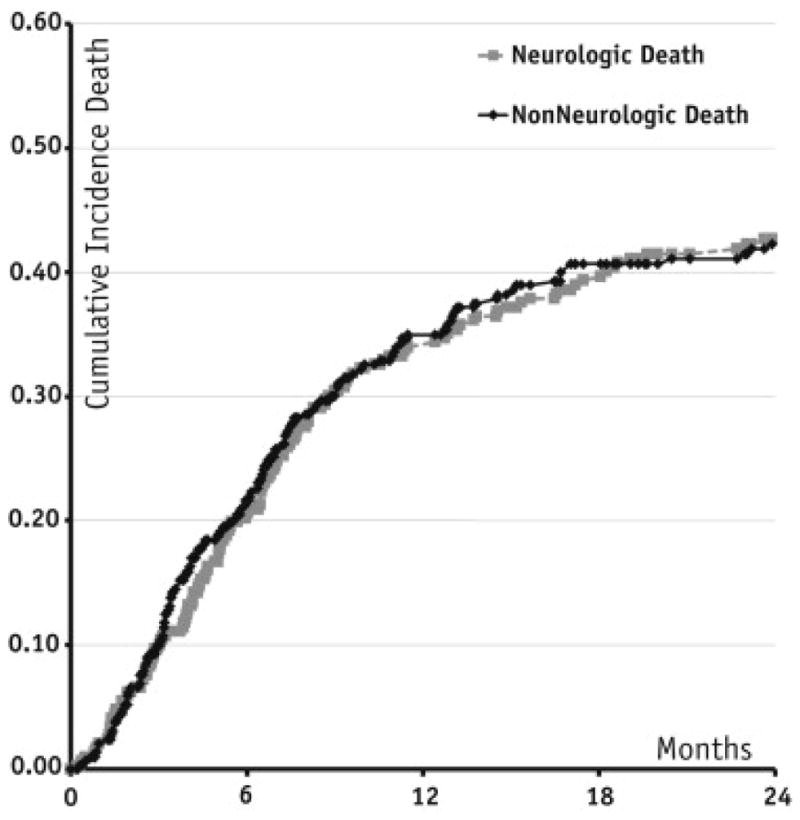
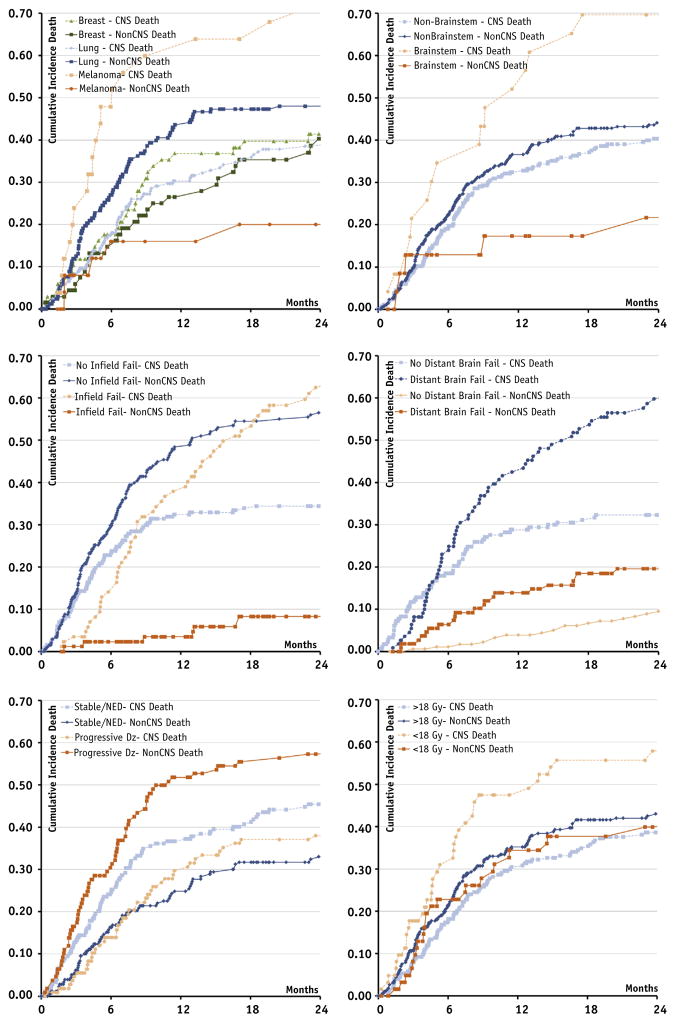
Results: The cumulative incidence of CNS and non-CNS death at 6 and 12 months was 20.6% and 21.6%, and 34.4% and 35%, respectively. Patients with melanoma histology (relative to breast) (aHR 2.7, 95% CI 1.5-5.0), brainstem location (aHR 2.1, 95% CI 1.3-3.5), and number of metastases (aHR 1.09, 95% CI 1.04-1.2) had increased aHR for CNS death. Progressive systemic disease (aHR 0.55, 95% CI 0.4-0.8) and increasing lowest margin dose (aHR 0.97, 95% CI 0.9-0.99) were protective against CNS death. Patients with lung histology (aHR 1.3, 95% CI 1.1-1.9) and progressive systemic disease (aHR 2.14, 95% CI 1.5-3.0) had increased aHR for non-CNS death.
Conclusion: Our nomogram provides individual estimates of neurologic death after salvage stereotactic radiosurgery for patients who have failed prior WBRT, based on histology, neuroanatomical location, age, lowest margin dose, and number of metastases after adjusting for their competing risk of death from other causes.
Published by Elsevier Inc.
Conflict of interest statement
Conflict of interest: none.
Figures
References
-
- Gaspar L, Scott C, Rotman M, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys. 1997;37:745–751. - PubMed
-
- Patchell RA, Tibbs PA, Regine WF, et al. Postoperative radiotherapy in the treatment of single metastases to the brain: A randomized trial. JAMA. 1998;280:1485–1489. - PubMed
-
- Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: A randomized controlled trial. JAMA. 2006;295:2483–2491. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
