

Advanced hepatocellular carcinoma and sorafenib: Diagnosis, indications, clinical and radiological follow-up
- PMID: 26052393
- PMCID: PMC4450181
- DOI: 10.4254/wjh.v7.i8.1041
Advanced hepatocellular carcinoma and sorafenib: Diagnosis, indications, clinical and radiological follow-up
Abstract
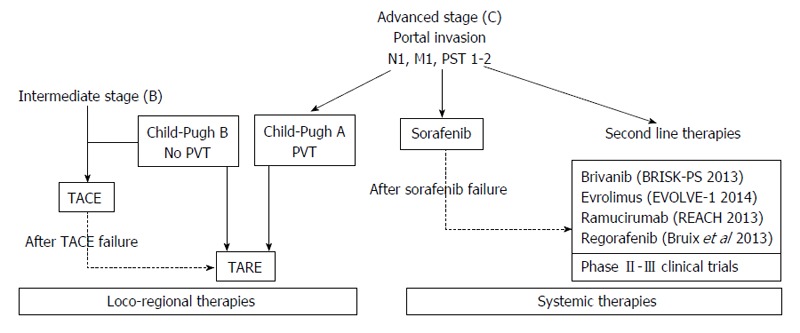
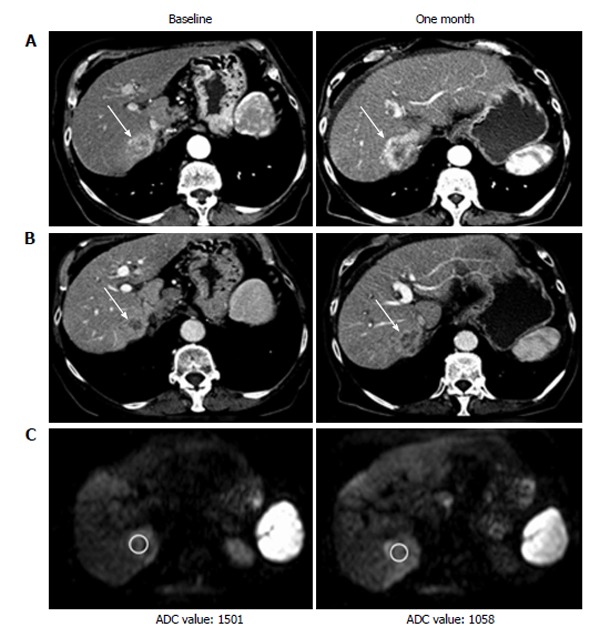
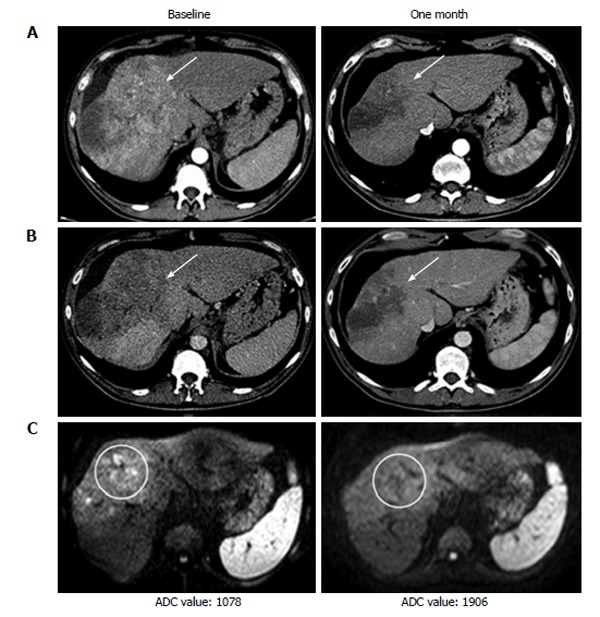
Advanced stage hepatocellular carcinoma (HCC) is a category of disease defined by radiological, clinical and hepatic function parameters, comprehending a wide range of patients with different general conditions. The main therapeutic option is represented by sorafenib treatment, a multi-kinase inhibitor with anti-proliferative and anti-angiogenic effect. Trans-arterial Radio Embolization also represents a promising new approach to intermediate/advanced HCC. Post-marketing clinical studies showed that only a portion of patients actually benefits from sorafenib treatment, and an even smaller percentage of patients treated shows partial/complete response on follow-up examinations, up against relevant costs and an incidence of drug related adverse effects. Although the treatment with sorafenib has shown a significant increase in mean overall survival in different studies, only a part of patients actually shows real benefits, while the incidence of drug related significant adverse effects and the economic costs are relatively high. Moreover, only a small percentage of patients also shows a response in terms of lesion dimensions reduction. Being able to properly differentiate patients who are responding to the therapy from non-responders as early as possible is then still difficult and could be a pivotal challenge for the future; in fact it could spare several patients a therapy often difficult to bear, directing them to other second line treatments (many of which are at the moment still under investigation). For this reason, some supplemental criteria to be added to the standard modified Response Evaluation Criteria in Solid Tumors evaluation are being searched for. In particular, finding some parameters (cellular density, perfusion grade and enhancement rate) able to predict the sensitivity of the lesions to anti-angiogenic agents could help in stratifying patients in terms of treatment responsiveness before the beginning of the therapy itself, or in the first weeks of sorafenib treatment. This would bring a strongly desirable help in clinical managements of these patients.
Keywords: Advanced hepatocellular carcinoma; Advanced hepatocellular carcinoma second line therapies; Barcelona clinic liver cancer; Diffusion weighted imaging; Hepatocellular carcinoma follow-up; Modified Response Evaluation Criteria in Solid Tumors; Perfusion weighted imaging; Response Evaluation Criteria in Solid Tumors; Response evaluation; Sorafenib.
Figures
References
-
- Caldwell S, Park SH. The epidemiology of hepatocellular cancer: from the perspectives of public health problem to tumor biology. J Gastroenterol. 2009;44 Suppl 19:96–101. - PubMed
-
- Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;379:1245–1255. - PubMed
-
- Cabibbo G, Enea M, Attanasio M, Bruix J, Craxì A, Cammà C. A meta-analysis of survival rates of untreated patients in randomized clinical trials of hepatocellular carcinoma. Hepatology. 2010;51:1274–1283. - PubMed
-
- European Association For The Study Of The Liver; European Organisation For Research And Treatment Of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56:908–943. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
