

The "Labral Bridge": A Novel Technique for Arthroscopic Anatomic Knotless Bankart Repair
- PMID: 26052499
- PMCID: PMC4454790
- DOI: 10.1016/j.eats.2014.11.010
The "Labral Bridge": A Novel Technique for Arthroscopic Anatomic Knotless Bankart Repair
Abstract
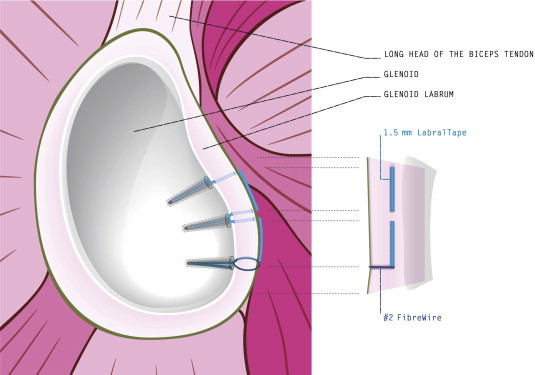
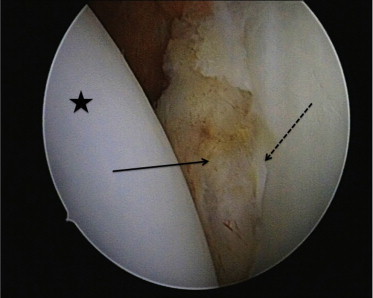
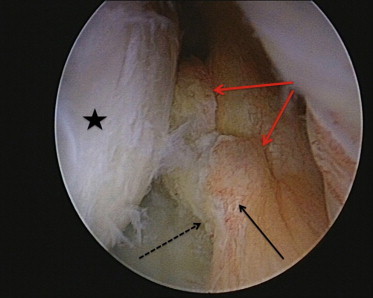
Arthroscopic Bankart repair with suture anchors is widely considered a mainstay for surgical treatment of anterior shoulder instability after recurrent anterior shoulder dislocations. Traditionally, the displaced capsulolabral complex is restored and firmly attached to the glenoid by placing multiple suture anchors individually from a 5- to 3-o'clock position. A variety of different techniques using different anchor designs and materials have been described. Knotless anchors are widely used nowadays for shoulder instability repair, providing a fast and secure way of labral fixation with favorable long-term outcomes. However, these techniques result in a concentrated point load of the reduced labrum to the glenoid at each suture anchor. We describe a technique, developed by the first author, using a 1.5-mm LabralTape (Arthrex, Naples, FL) in combination with knotless suture anchors (3.5-mm PEEK [polyether ether ketone] PushLock anchors; Arthrex), for hybrid fixation of the labrum. The LabralTape is used to secure the torn labrum to the glenoid between each suture anchor, thus potentially providing a more even pressure distribution.
Figures
References
-
- Bankart A.S., Cantab M.C. Recurrent or habitual dislocation of the shoulder-joint. 1923. Clin Orthop Relat Res. 1993;(291):3–6. - PubMed
-
- Rowe C.R., Patel D., Southmayd W.W. The Bankart procedure: A long-term end-result study. J Bone Joint Surg Am. 1978;60:1–16. - PubMed
-
- Pope E.J., Ward J.P., Rokito A.S. Anterior shoulder instability—A history of arthroscopic treatment. Bull NYU Hosp Jt Dis. 2011;69:44–49. - PubMed
-
- Cole B.J., Romeo A.A. Arthroscopic shoulder stabilization with suture anchors: Technique, technology, and pitfalls. Clin Orthop Relat Res. 2001;(390):17–30. - PubMed
-
- Ng D.Z., Kumar V.P. Arthroscopic Bankart repair using knot-tying versus knotless suture anchors: Is there a difference? Arthroscopy. 2014;30:422–427. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
