

The impact of obesity on the relationship between epicardial adipose tissue, left ventricular mass and coronary microvascular function
- PMID: 26054890
- PMCID: PMC4521095
- DOI: 10.1007/s00259-015-3087-5
The impact of obesity on the relationship between epicardial adipose tissue, left ventricular mass and coronary microvascular function
Abstract
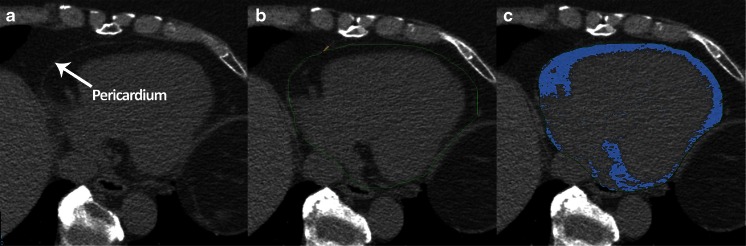
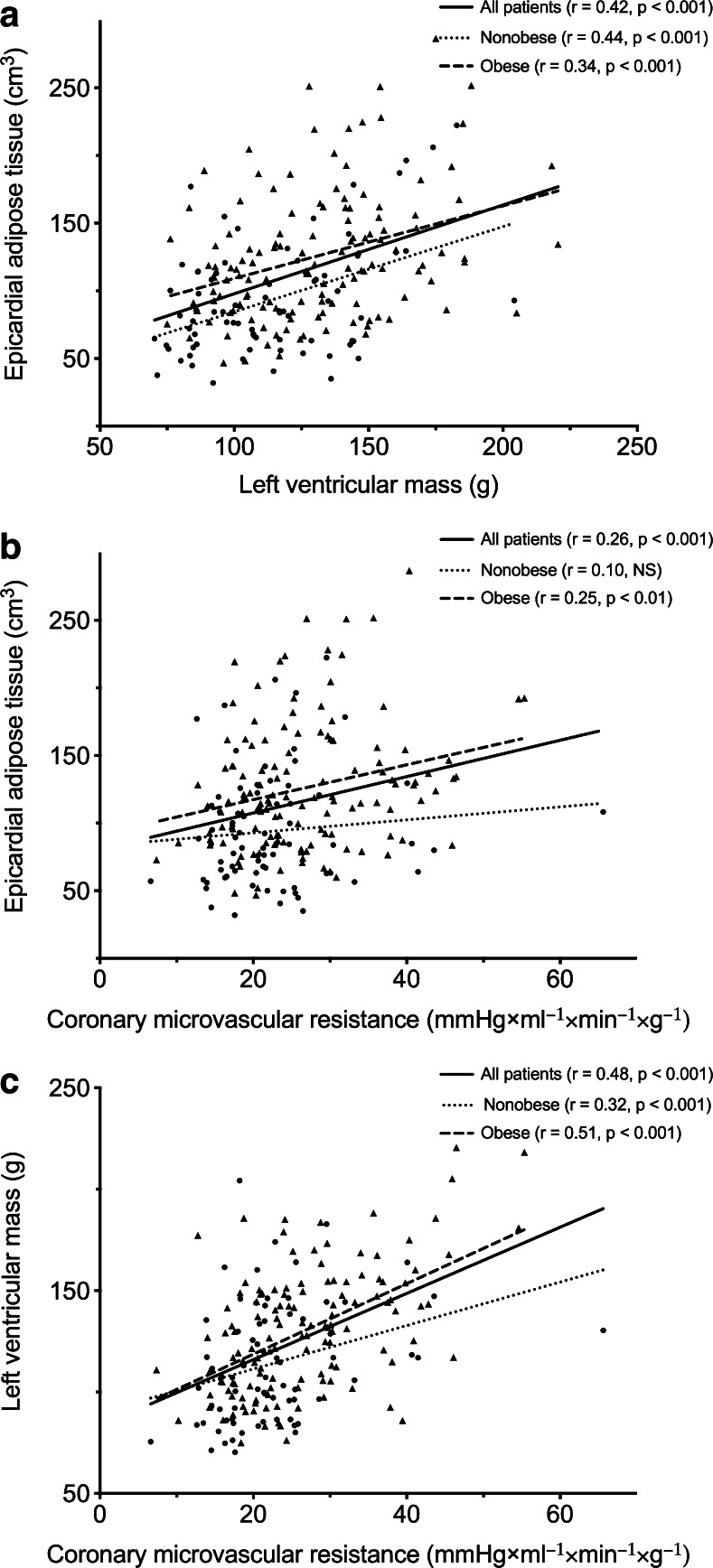
Purpose: Epicardial adipose tissue (EAT) has been linked to coronary artery disease (CAD) and coronary microvascular dysfunction. However, its injurious effect may also impact the underlying myocardium. This study aimed to determine the impact of obesity on the quantitative relationship between left ventricular mass (LVM), EAT and coronary microvascular function.
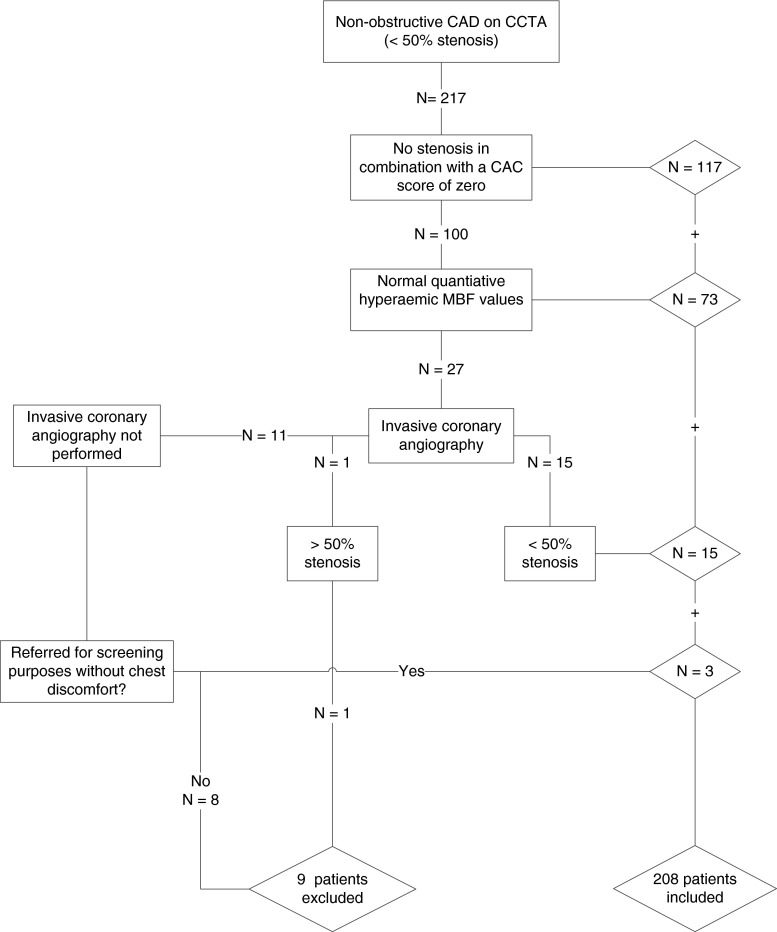
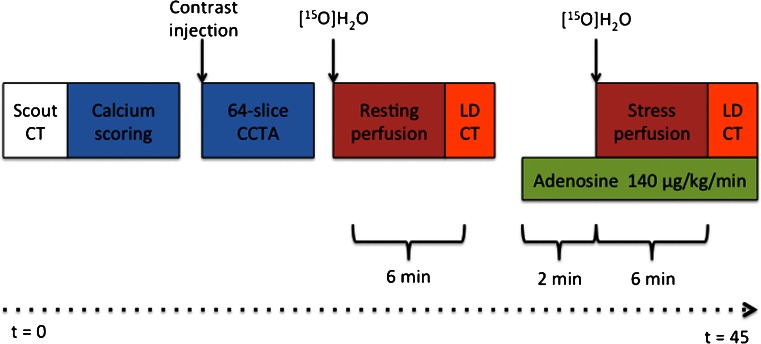
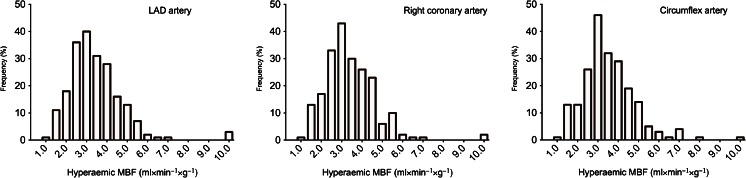
Methods: A total of 208 (94 men, 45 %) patients evaluated for CAD but free of coronary obstructions underwent quantitative [(15)O]H2O hybrid positron emission tomography (PET)/CT imaging. Coronary microvascular resistance (CMVR) was calculated as the ratio of mean arterial pressure to hyperaemic myocardial blood flow.
Results: Obese patients [body mass index (BMI) > 25, n = 133, 64 % of total] had more EAT (125.3 ± 47.6 vs 93.5 ± 42.1 cc, p < 0.001), a higher LVM (130.1 ± 30.4 vs 114.2 ± 29.3 g, p < 0.001) and an increased CMVR (26.6 ± 9.1 vs 22.3 ± 8.6 mmHg×ml(-1)×min(-1)×g(-1), p < 0.01) as compared to nonobese patients. Male gender (β = 40.7, p < 0.001), BMI (β = 1.61, p < 0.001), smoking (β = 6.29, p = 0.03) and EAT volume (β = 0.10, p < 0.01) were identified as independent predictors of LVM. When grouped according to BMI status, EAT was only independently associated with LVM in nonobese patients. LVM, hypercholesterolaemia and coronary artery calcium score were independent predictors of CMVR.
Conclusion: EAT volume is associated with LVM independently of BMI and might therefore be a better predictor of cardiovascular risk than BMI. However, EAT volume was not related to coronary microvascular function after adjustments for LVM and traditional risk factors.
Figures
References
-
- Rosito GA, Massaro JM, Hoffmann U, Ruberg FL, Mahabadi AA, Vasan RS, et al. Pericardial fat, visceral abdominal fat, cardiovascular disease risk factors, and vascular calcification in a community-based sample: the Framingham Heart Study. Circulation. 2008;117:605–613. doi: 10.1161/CIRCULATIONAHA.107.743062. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
