

Stage, age, and EBV status impact outcomes of plasmablastic lymphoma patients: a clinicopathologic analysis of 61 patients
- PMID: 26055271
- PMCID: PMC4472407
- DOI: 10.1186/s13045-015-0163-z
Stage, age, and EBV status impact outcomes of plasmablastic lymphoma patients: a clinicopathologic analysis of 61 patients
Abstract
Background: Plasmablastic lymphoma (PBL) is a rare aggressive neoplasm with lymphoid and plasmacytic differentiation that is commonly associated with immunodeficiency and an unfavorable prognosis. Clinicopathologic features have been largely derived from cases reports and small series with limited outcome analyses.
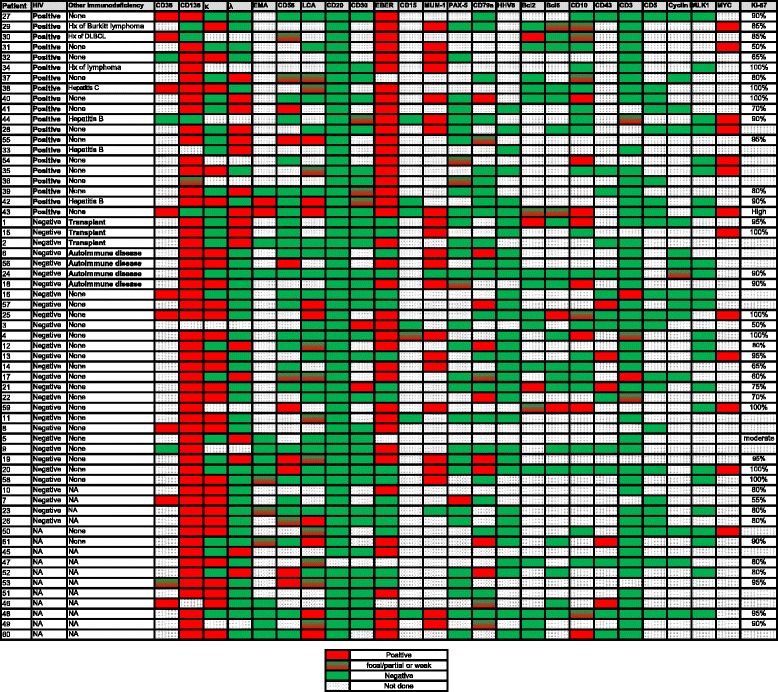
Patients and methods: The demographic, clinicopathologic features, and clinical outcomes of a cohort of 61 patients with PBL were reviewed and analyzed.
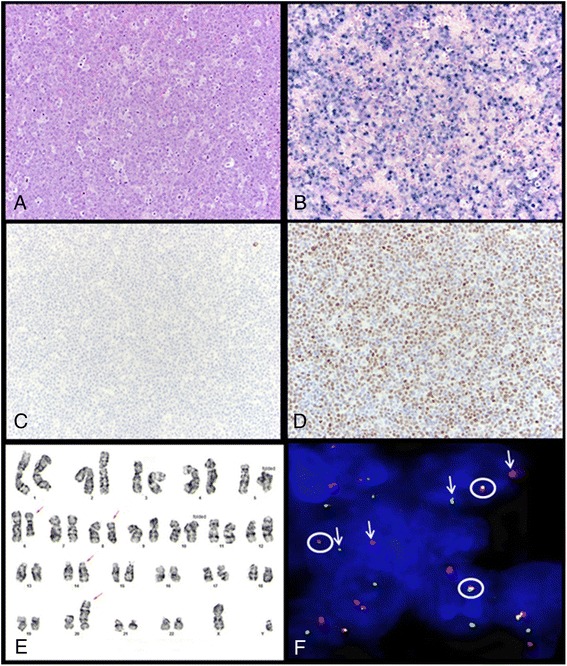
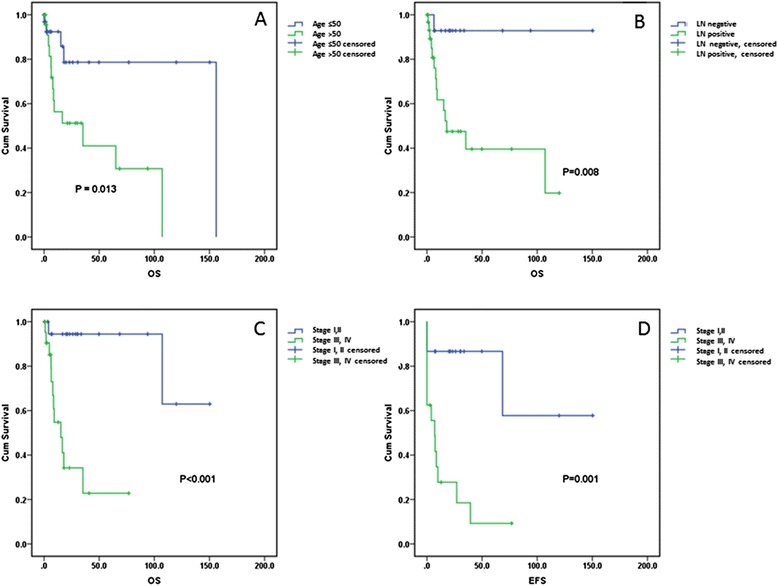
Results: Patients had a median age of 49 years (range 21-83 years) and most (49/61; 80%) were men. Human immunodeficiency virus (HIV) status was available for 50 patients: 20 were HIV-positive and 30 HIV-negative. Twenty-three patients were immunocompetent. Abdominal/gastrointestinal complaints were the most common presenting symptoms, reported in 14 of 47 (30%) of patients. At presentation, 24 of 43 (56%) patients had stage III or IV disease. Epstein-Barr virus (EBV) was detected in 40 of 57 (70%) cases. MYC rearrangement was identified in 10/15 (67%) cases assessed, and MYC overexpression was seen in all cases assessed regardless of MYC rearrangement status. HIV-positive patients were significantly younger than those who were HIV-negative (median 42 vs. 58 years; p = 0.006). HIV-positive patients were also significantly more likely to have EBV-positive disease compared with HIV-negative patients (19/19, 100% vs. 15/29, 52%; p = 0.002). Patients who received CHOP chemotherapy tended to have better overall survival (OS) compared with those who received hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (hyper-CVAD) (p = 0.078). HIV status had no impact on OS. Patients with EBV-positive PBL had a better event-free survival (EFS) (p = 0.047) but not OS (p = 0.306). Notably, OS was adversely impacted by age ≥ 50 years (p = 0.013), stage III or IV disease (p = <0.001), and lymph node involvement (p = 0.008).
Conclusions: The most significant prognostic parameters in patients with PBL are age, stage, and, to a lesser extent, EBV status. In this study, two-thirds of PBL cases assessed were associated with MYC rearrangement and all showed MYC overexpression.
Figures
References
-
- Stein H, Harris NL, Campo E, et al. Plasmablastic lymphoma. In: Swerdlow SH, Campo E, Harris NL, et al., editors. WHO classification of tumours of haematopoietic and lymphoid tissues. Lyon: IARC; 2008. pp. 256–7.
-
- Miranda RN, Khoury JD, Medeiros LJ. Atlas of Lymph Node Pathology. New York: Springer; 2014. Plasmablastic Lymphoma; pp. 265–8.
-
- Morscio J, Dierickx D, Nijs J, et al. Clinicopathologic comparison of plasmablastic lymphoma in HIV-positive, immunocompetent, and posttransplant patients: single-center series of 25 cases and meta-analysis of 277 reported cases. Am J Surg Pathol. 2014;38:875–86. doi: 10.1097/PAS.0000000000000234. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
