

Nomogram predicted survival of patients with adenocarcinoma of esophagogastric junction
- PMID: 26055624
- PMCID: PMC4465317
- DOI: 10.1186/s12957-015-0613-7
Nomogram predicted survival of patients with adenocarcinoma of esophagogastric junction
Abstract
Background: The aim of this study is to develop a prognostic nomogram for patients with adenocarcinoma of esophagogastric junction and compare its predictive accuracy with the traditional tumor-node-metastasis (TNM) malignant staging system.
Methods: Patients from the Surveillance, Epidemiology, and End Results Program (from 1988 to 2011) and the First Affiliated Hospital of Xi'an Jiaotong University (from 2005 to 2010) were collected retrospectively. Preselected multiple potential interactions were tested irrespective of significance as nomogram parameters. And the Harrell's C-index was used to estimate the accuracy of the nomogram system. Model validation was performed using bootstrap to quantify our modeling strategy.
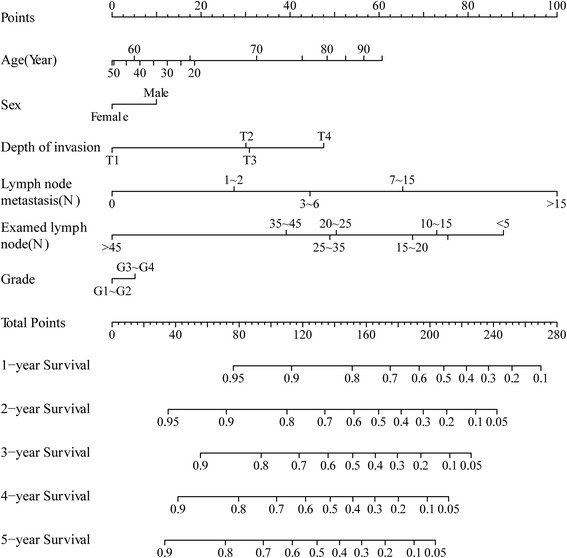
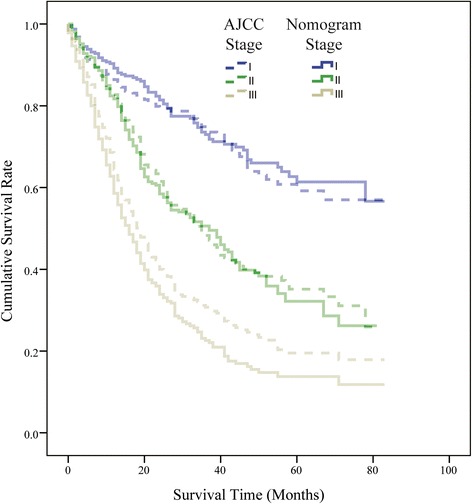
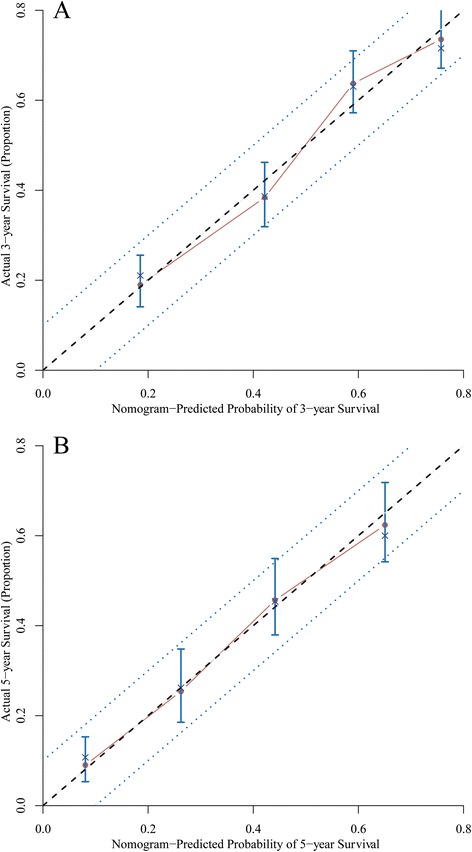
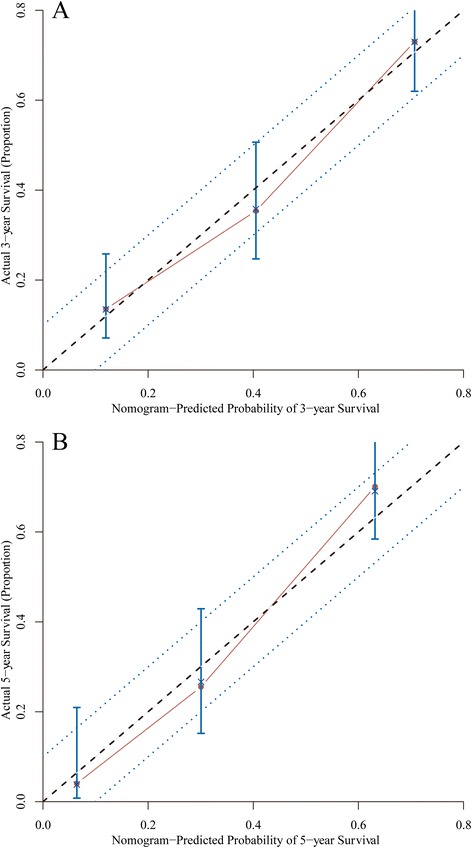
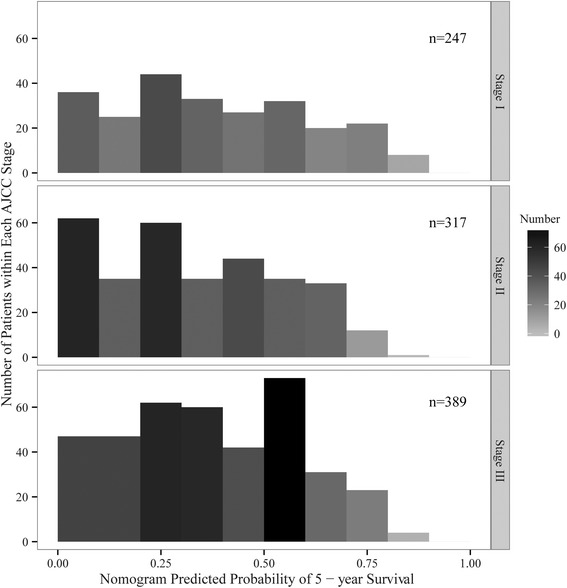
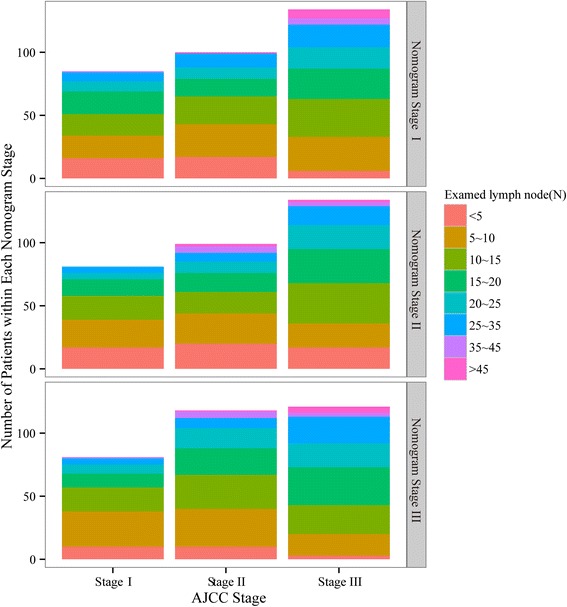
Results: In our study, six clinical associated factors (age, sex, depth of invasion, metastasized lymph nodes, examined lymph nodes, histological grade) were evaluated in the nomogram. In the training set, the nomogram exhibited superior discrimination power compared with the American Joint Committee on Cancer (AJCC) TNM classification (Harrell's C-index, 0.69 and 0.63, respectively). Calibration of the nomogram predicted survival was similar to the actual overall survival. In the validation set, the discrimination of nomogram was also better than the AJCC TNM staging system (C-index, 0.75 and 0.65, respectively), and the calibration of nomogram predicted survival was within a 10 % margin of actual overall survival.
Conclusions: Based on the patients with adenocarcinoma of esophagogastric junction from a Western and an Eastern database, the nomogram provided significantly improved discrimination than the traditional AJCC TNM classification and also provided an accurate individualized prediction of the survival.
Figures

References
-
- Sobin LH, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumours. New York: John Wiley & Sons; 2011.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
