

Review
doi: 10.1161/CIRCULATIONAHA.114.006980.
Emerging Concepts in the Molecular Basis of Pulmonary Arterial Hypertension: Part II: Neurohormonal Signaling Contributes to the Pulmonary Vascular and Right Ventricular Pathophenotype of Pulmonary Arterial Hypertension
Affiliations
- PMID: 26056345
- PMCID: PMC4465126
- DOI: 10.1161/CIRCULATIONAHA.114.006980
Item in Clipboard
Review
Emerging Concepts in the Molecular Basis of Pulmonary Arterial Hypertension: Part II: Neurohormonal Signaling Contributes to the Pulmonary Vascular and Right Ventricular Pathophenotype of Pulmonary Arterial Hypertension
Circulation.
.
No abstract available
Keywords: aldosterone; angiotensins; catecholamines; heart ventricles; hypertension; pulmonary.
Conflict of interest statement
Figures
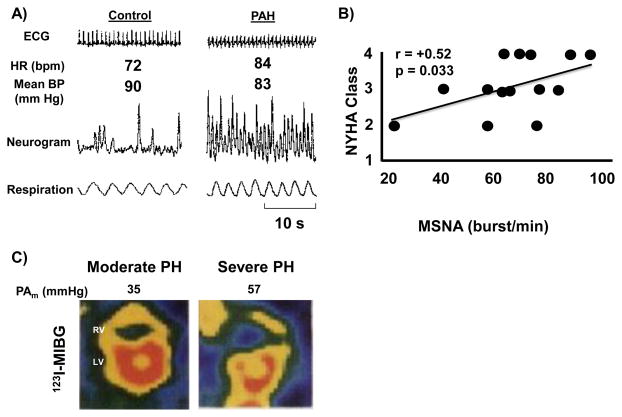
Sympathetic nervous system activation is increased in pulmonary arterial hypertension (PAH). (A) Muscle sympathetic nerve activity neurograms demonstrate increased sympathetic nerve traffic in skeletal muscle of PAH patients compared to controls. (B) This correlates with more severe heart failure symptoms as assessed by the New York Heart Association (NYHA) functional class. (C) Cardiac imaging with 123I- metaiodobenzylguanidine (MIBG), a norepinephrine analog that competes with norepinephrine for uptake, showing a reduction in 123I-MIBG uptake (i.e., higher norepinephrine uptake) in the RV of a patient with severe pulmonary hypertension. HR, heart rate; BP, blood pressure; s, seconds, PH, pulmonary hypertension. Reproduced with permission from references , .
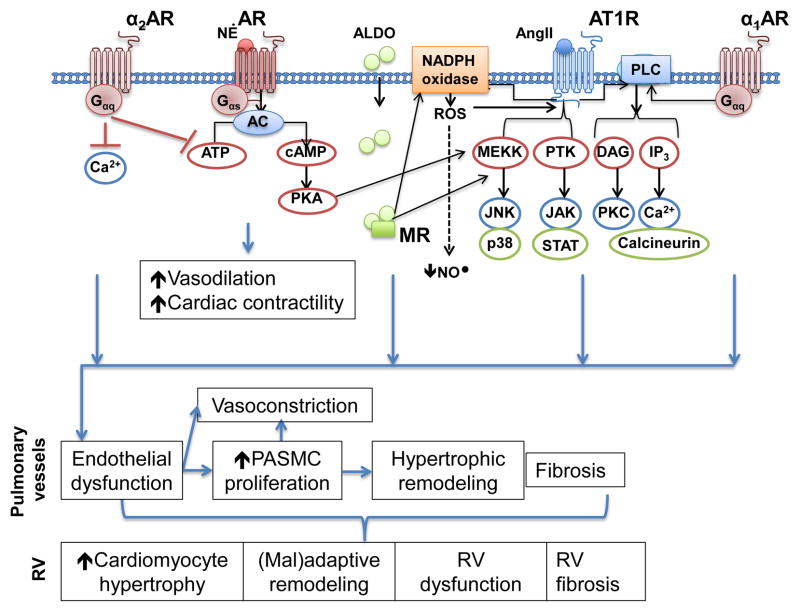
Adrenergic receptor signaling and cross-talk with the renin-angiotensin aldosterone system. Activation of β-adrenergic receptor signaling increases cAMP levels and activates protein kinase A (PKA) to promote vasodilation and an increase in cardiac contractility. These effects are opposed by α2-AR signaling. PKA also activates the MAP kinase signaling pathway, which is downstream from the angiotensin type 1 receptor (AT1R). AT1R also activates protein tyrosine kinases (PTK), which have been implicated in pulmonary hypertension, and similar to α1-AR, activates phospholipase C (PLC). Both AT1R and mineralocorticoid receptor (MR) activate NADPH oxidase to increase reactive oxygen species formation (ROS), which decrease bioavailable nitric oxide (NO•).
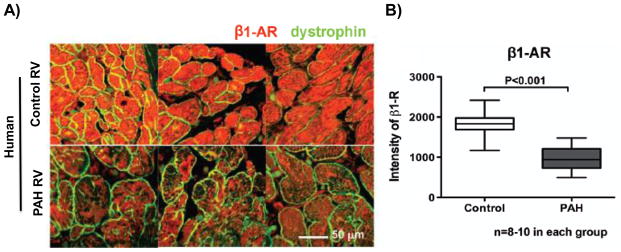
β1-adrenergic receptor expression is down regulated in the right ventricle (RV) of patients with pulmonary arterial hypertension (PAH). (A) A representative cross-sectional image of RV cardiomyocytes and (B) mean values from human tissue microarrays showing down regulation of the β1-adrenergic receptor in hypertrophied RVs from patients with PAH compared to age- and sex-matched controls. Reproduced with permission from reference .
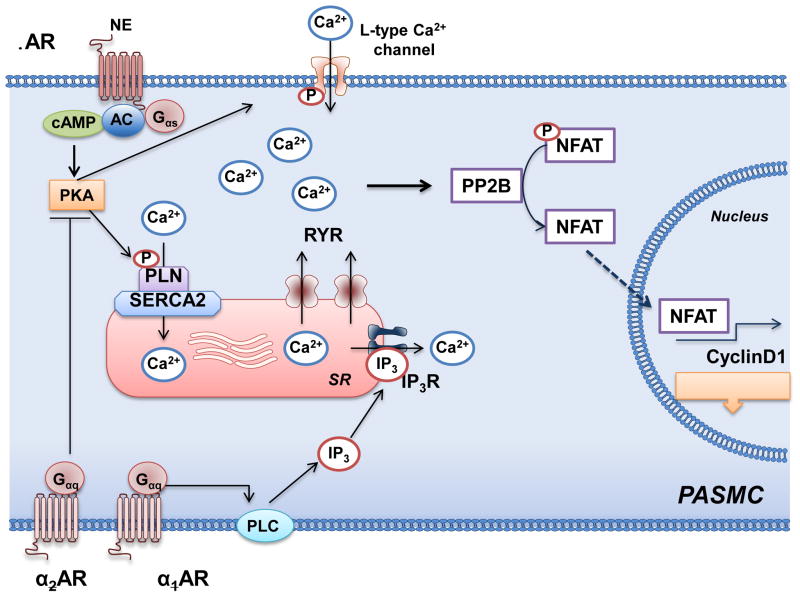
Adrenergic receptor signaling, intracellular calcium, and pulmonary artery smooth muscle cell proliferation. In pulmonary artery smooth muscle cells (PASMC), β-adrenergic receptor (AR) activates adenylyl cyclase (AC) to increase cAMP and, thereby, activate protein kinase A (PKA). PKA phosphorylates phospholamban (PLN) and increase activity of the sarcoplasmic reticulum Ca2+-ATPase (SERCA2), which decreases intracellular Ca2+ levels. In pulmonary hypertension, SERCA2 expression is downregulated. This results in high intracellular Ca2+ levels through the actions of the ryanodine receptors (RYR) and α-AR signaling. The elevated levels of intracellular Ca2+ stimulate proliferation through protein phosphatase 2B (PP2B), translocation of nuclear factor of activated T cells (NFAT) to the nucleus to promote transcription of cyclin D1. PLC, phospholipase C, inositol triphosphate.
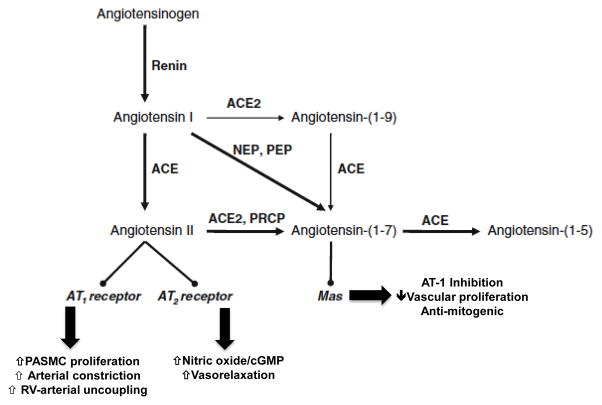
Angiotensin II and related metabolites. Angiotensin II is generated from angiotensin I via the actions of angiotensin converting enzyme (ACE). Angiotensin I and II may also be metabolized to the vasoactive heptapeptides angiotensin-(1-9) and angiotensin-(1-7) through the actions of angiotensin converting enzyme 2 (ACE2) and neutral endopeptidsase (NEP) and prolylendopeptidase (PEP). Angiotensin II may stimulate angiotensin type-1 (AT-1) receptors to increase pulmonary artery smooth muscle cell (PASMC) proliferation, vasoconstriction, and disrupt right ventricular (RV)-arterial coupling. By contrast, stimulation of angiotensin II receptor type 2 (AT-2) or the Mas receptor by angiotensin II or angiotensin-(1-7) is associated with vasculoprotective effects, including increased nitric oxide generation and a decrease in cell proliferation and vasodilation. PRCP, prolylcarboxypeptidase. Adapted with modifications from reference .
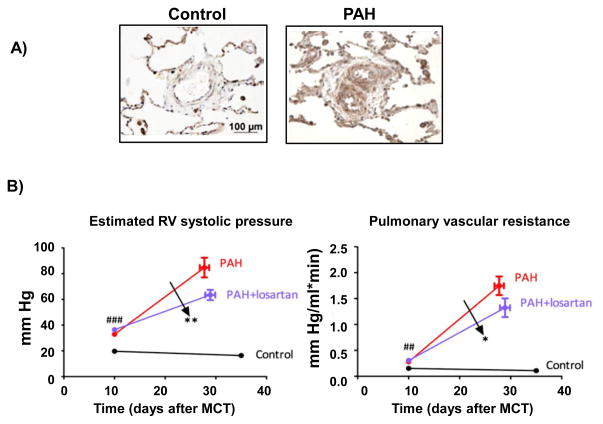
Angiotensin II type-1 receptor (AT1R) inhibition improves hemodynamics in pulmonary arterial hypertension (PAH). (A) Expression levels of AT1R are increased in pulmonary arterioles harvested from patients with idiopathic PAH compared to controls. (B) Inhibition of AT1R with losartan (20 mg/kg) improves RV systolic pressure (left) and pulmonary vascular resistance (right) in monocrotaline-PAH. Reprinted from Ref. with permission of the American Thoracic Society. Copyright ©2014 American Thoracic Society
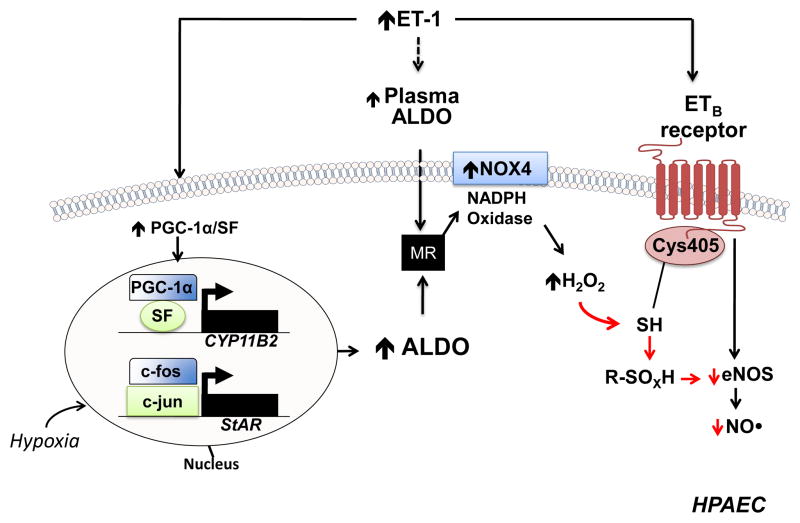
A proposed mechanism by which hyperaldosteronism decreases pulmonary endothelial eNOS activation and nitric oxide (NO•) generation in PAH. Hyperaldosteronism (ALDO) in pulmonary arterial hypertension (PAH) may occur via i) endothelin-1 (ET-1)-mediated activation of PPARγ coactivator-1α (PGC-1α)/steroidogenesis factor-1 (SF) to increase CYP11B2 (aldosterone synthase) gene transcription in human pulmonary artery endothelial cells (HPAECs); ii) hypoxia-stimulated upregulation of steroidogenic acute regulatory protein (StAR) by increasing binding of c-fos and c-jun to the promoter; and, iii) adrenal ALDO synthesis via ET-1 and/or overactivation of the renin-angiotensin pathway. Stimulation of the mineralocorticoid receptor (MR) in HPAECs by ALDO activates NADPH oxidase type 4 (NOX4) to increase levels of hydrogen peroxide (H2O2), which, in turn, oxidatively modifies redox sensitive, functional cysteinyl thiol(s) in the ETB receptor (Cys405) to impair ETB-dependent activation of eNOS and decrease synthesis of nitric oxide (NO•). eNOS, endothelial nitric oxide synthase; R-SOXH, higher oxidative intermediaries of cysteine. Adapted from ref .
References
-
- O’Rourke MF, Yaginuma T, Avolio AP. Physiological and pathophysiological implications of ventricular/vascular coupling. Ann Biomed Eng. 1984;12:119–134. - PubMed
-
- Vonk-Noordegraaf A, Westerhof N. Describing right ventricular function. Eur Respir J. 2013;41:1419–1423. - PubMed
-
- Forfia PR, Fisher MR, Mathai SC, Housten-Harris T, Hemnes AR, Borlaug BA, Chamera E, Corretti MC, Champion HC, Abraham TP, Girgis RE, Hassoun PM. Tricuspid annular displacement predicts survival in pulmonary hypertension. Am J Respir Crit Care Med. 2006;174:1034–1041. - PubMed
-
- Mehra MR, Park MH, Landzberg MJ, Lala A, Waxman AB. Right heart failure: toward a common language. J Heart Lung Transplant. 2014;33:123–126. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
