

Reductions in post-hepatectomy liver failure and related mortality after implementation of the LiMAx algorithm in preoperative work-up: a single-centre analysis of 1170 hepatectomies of one or more segments
- PMID: 26058324
- PMCID: PMC4474514
- DOI: 10.1111/hpb.12424
Reductions in post-hepatectomy liver failure and related mortality after implementation of the LiMAx algorithm in preoperative work-up: a single-centre analysis of 1170 hepatectomies of one or more segments
Abstract
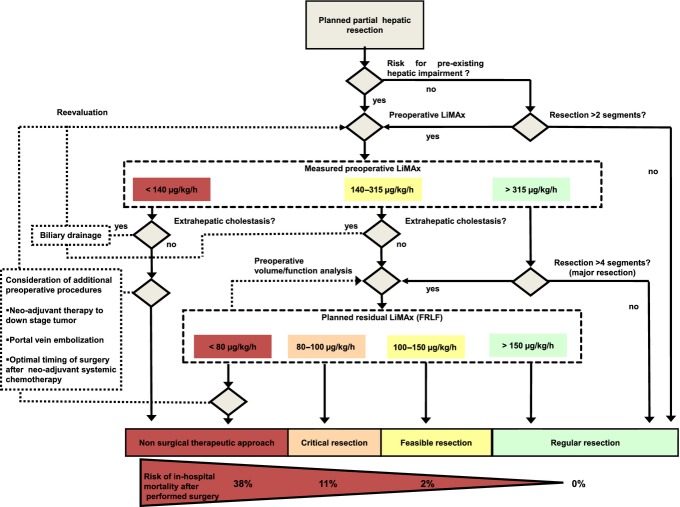
Objectives: Post-hepatectomy liver failure has a major impact on patient outcome. This study aims to explore the impact of the integration of a novel patient-centred evaluation, the LiMAx algorithm, on perioperative patient outcome after hepatectomy.
Methods: Trends in perioperative variables and morbidity and mortality rates in 1170 consecutive patients undergoing elective hepatectomy between January 2006 and December 2011 were analysed retrospectively. Propensity score matching was used to compare the effects on morbidity and mortality of the integration of the LiMAx algorithm into clinical practice.
Results: Over the study period, the proportion of complex hepatectomies increased from 29.1% in 2006 to 37.7% in 2011 (P = 0.034). Similarly, the proportion of patients with liver cirrhosis selected for hepatic surgery rose from 6.9% in 2006 to 11.3% in 2011 (P = 0.039). Despite these increases, rates of post-hepatectomy liver failure fell from 24.7% in 2006 to 9.0% in 2011 (P < 0.001) and liver failure-related postoperative mortality decreased from 4.0% in 2006 to 0.9% in 2011 (P = 0.014). Propensity score matching was associated with reduced rates of post-hepatectomy liver failure [24.7% (n = 77) versus 11.2% (n = 35); P < 0.001] and related mortality [3.8% (n = 12) versus 1.0% (n = 3); P = 0.035].
Conclusions: Postoperative liver failure and postoperative liver failure-related mortality decreased in patients undergoing hepatectomy following the implementation of the LiMAx algorithm.
© 2015 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Belghiti J, Hiramatsu K, Benoist S, Massault P, Sauvanet A, Farges O. Seven hundred forty-seven hepatectomies in the 1990s: an update to evaluate the actual risk of liver resection. J Am Coll Surg. 2000;191:38–46. - PubMed
-
- Clavien PA, Petrowsky H, DeOliveira ML, Graf R. Strategies for safer liver surgery and partial liver transplantation. N Engl J Med. 2007;356:1545–1559. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
