

Regional (spinal, epidural, caudal) versus general anaesthesia in preterm infants undergoing inguinal herniorrhaphy in early infancy
- PMID: 26058963
- PMCID: PMC6885061
- DOI: 10.1002/14651858.CD003669.pub2
Regional (spinal, epidural, caudal) versus general anaesthesia in preterm infants undergoing inguinal herniorrhaphy in early infancy
Abstract
Background: With improvements in neonatal intensive care, more preterm infants are surviving the neonatal period and presenting for surgery in early infancy. Inguinal hernia is the most common condition requiring early surgery, appearing in 38% of infants whose birth weight is between 751 grams and 1000 grams. Approximately 20% to 30% of otherwise healthy preterm infants having general anaesthesia for inguinal hernia surgery at a postmature age have at least one apnoeic episode within the postoperative period. Research studies have failed to adequately distinguish the effects of apnoeic episodes from other complications of extreme preterm gestation on the risk of brain injury, or to investigate the potential impact of postoperative apnoea upon longer term neurodevelopment. In addition to episodes of apnoea, there are concerns that anaesthetic and sedative agents may have a direct toxic effect on the developing brain of preterm infants even after reaching postmature age. It is proposed that regional anaesthesia may reduce the risk of postoperative apnoea, avoid the risk of anaesthetic-related neurotoxicity and improve neurodevelopmental outcomes in preterm infants requiring surgery for inguinal hernia at a postmature age.
Objectives: To determine if regional anaesthesia reduces postoperative apnoea, bradycardia, the use of assisted ventilation, and neurological impairment, in comparison to general anaesthesia, in preterm infants undergoing inguinal herniorrhaphy at a postmature age.
Search methods: The following databases and resources were searched: the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, 2015, Issue 2), MEDLINE (December 2002 to 25 February 2015), EMBASE (December 2002 to 25 February 2015), controlled-trials.com and clinicaltrials.gov, reference lists of published trials and abstracts published in Pediatric Research and Pediatric Anesthesia.
Selection criteria: Randomised and quasi-randomised controlled trials of regional (spinal, epidural, caudal) versus general anaesthesia, or combined regional and general anaesthesia, in former preterm infants undergoing inguinal herniorrhaphy in early infancy.
Data collection and analysis: At least two of three review authors (LJ, JF, AL) independently extracted data and performed analyses. Authors were contacted to obtain missing data. The methodological quality of each study was assessed according to the criteria of the Cochrane Neonatal Review Group. Data were analysed using Review Manager 5. Meta-analyses were performed with calculation of risk ratios (RR) and risk difference (RD), along with their 95% confidence intervals (CI) where appropriate.
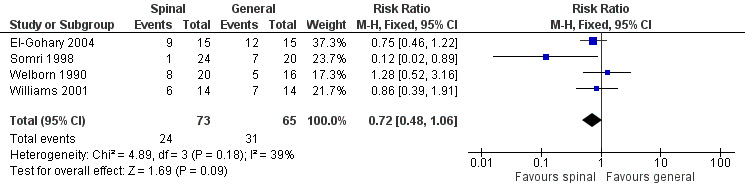
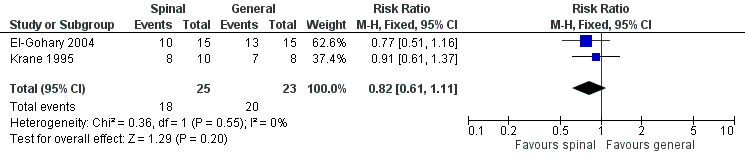
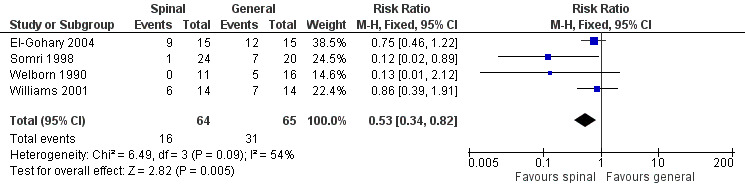
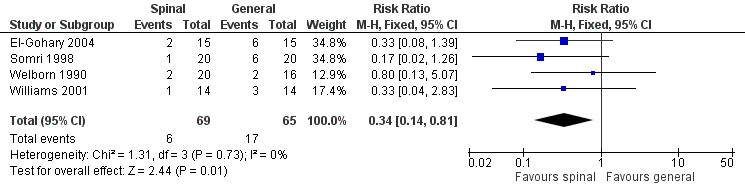
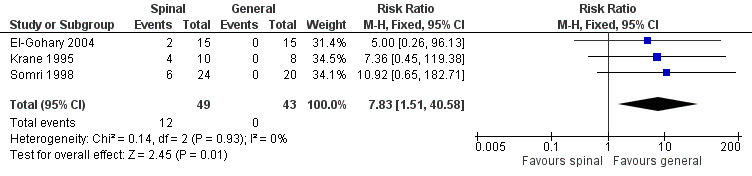
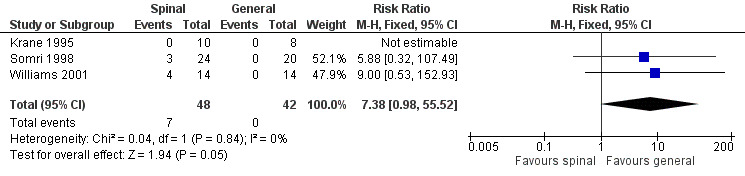
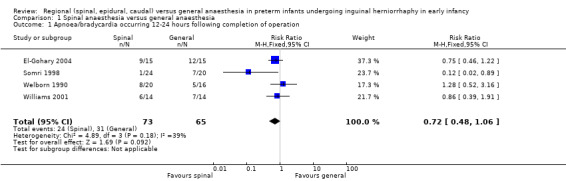
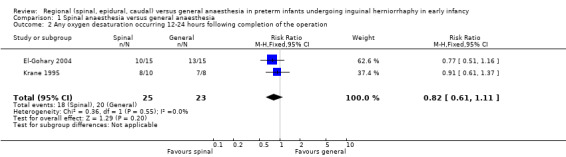
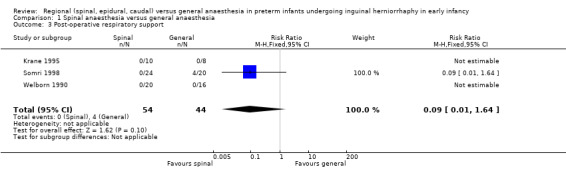
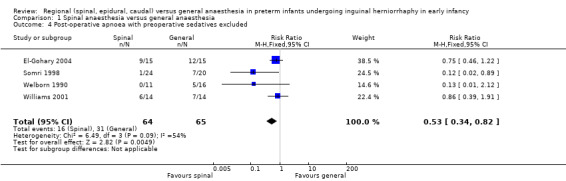
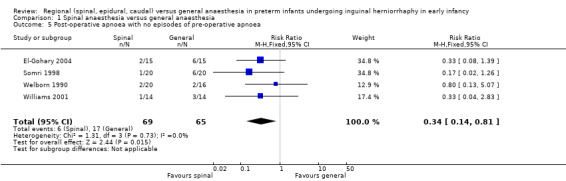
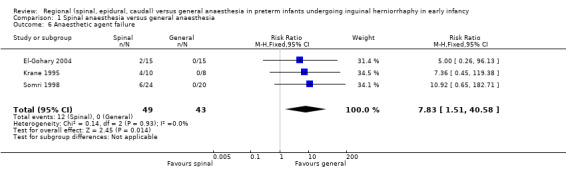
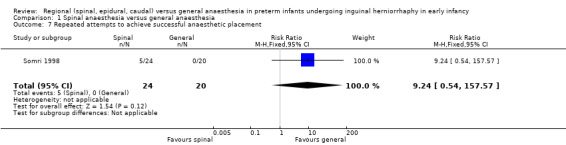
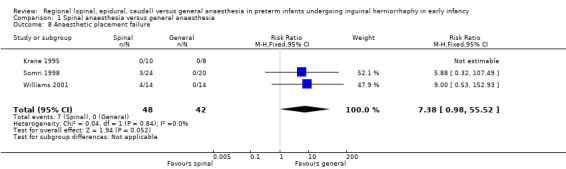
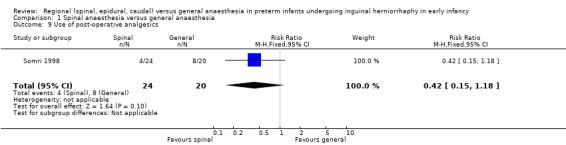
Main results: Seven small trials comparing spinal with general anaesthesia in the repair of inguinal hernia were identified. Two trial reports are listed as 'Studies awaiting classification' due to insufficient information on which to base an eligibility assessment. There was no statistically significant difference in the risk of postoperative apnoea/bradycardia (typical RR 0.72, 95% CI 0.48 to 1.06; 4 studies, 138 infants), postoperative oxygen desaturation (typical RR 0.82, 95% CI 0.61 to 1.11; 2 studies, 48 infants), the use of postoperative analgesics (RR 0.42, 95% CI 0.15 to 1.18; 1 study, 44 infants), or postoperative respiratory support (typical RR 0.09, 95% CI 0.01 to1.64; 3 studies, 98 infants) between infants receiving spinal or general anaesthesia. When infants who had received preoperative sedatives were excluded, the meta-analysis supported a reduction in the risk of postoperative apnoea in the spinal anaesthesia group (typical RR 0.53, 95% CI 0.34 to 0.82; 4 studies, 129 infants). Infants with no history of apnoea in the preoperative period and receiving spinal anaesthesia (including a subset of infants who had received sedatives) had a reduced risk of postoperative apnoea and this reached statistical significance (typical RR 0.34, 95% CI 0.14 to 0.81; 4 studies, 134 infants). Infants receiving spinal rather than general anaesthesia had a statistically significant increased risk of anaesthetic agent failure (typical RR 7.83, 95% CI 1.51 to 40.58; 3 studies, 92 infants). Infants randomised to receive spinal anaesthesia had an increased risk of anaesthetic placement failure of borderline statistical significance (typical RR 7.38, 95% CI 0.98 to 55.52; typical RD 0.15, 95% CI 0.03 to 0.27; 3 studies, 90 infants).
Authors' conclusions: There is moderate-quality evidence to suggest that the administration of spinal in preference to general anaesthesia without pre- or intraoperative sedative administration may reduce the risk of postoperative apnoea by up to 47% in preterm infants undergoing inguinal herniorrhaphy at a postmature age. For every four infants treated with spinal anaesthesia, one infant may be prevented from having an episode of postoperative apnoea (NNTB=4). In those infants without preoperative apnoea, there is low-quality evidence that spinal rather than general anaesthesia may reduce the risk of preoperative apnoea by up to 66%. There was no difference in the effect of spinal compared with general anaesthesia on the overall incidence of postoperative apnoea, bradycardia, oxygen desaturation, need for postoperative analgesics or respiratory support. Limitations on these results included varying use of sedative agents, or different anaesthetic agents, or combinations of these factors, in addition to trial quality aspects such as allocation concealment and inadequate blinding of intervention and outcome assessment. The meta-analyses may have inadequate power to detect a difference between groups for some outcomes, with estimates of effect based on a total population of fewer than 140 infants.The effect of newer, rapidly acting, quickly metabolised general anaesthetic agents on safety with regard to the risk of postoperative apnoea and neurotoxic exposure has not so far been established in randomised trials. There is potential for harm from postoperative apnoea and direct brain toxicity from general anaesthetic agents superimposed upon pre-existing altered brain development in infants born at very to extreme preterm gestation. This highlights the clear need for the examination of neurodevelopmental outcomes in the context of large randomised controlled trials of general, compared with spinal, anaesthesia, in former preterm infants undergoing surgery for inguinal hernia.There is a particular need to examine the impact of the choice of spinal over general anaesthesia on respiratory and neurological outcomes in high-risk infant subgroups with severe respiratory disease and previous brain injury.
Conflict of interest statement
None
Figures
Update of
-
Regional (spinal, epidural, caudal) versus general anaesthesia in preterm infants undergoing inguinal herniorrhaphy in early infancy.Cochrane Database Syst Rev. 2003;(3):CD003669. doi: 10.1002/14651858.CD003669. Cochrane Database Syst Rev. 2003. Update in: Cochrane Database Syst Rev. 2015 Jun 09;(6):CD003669. doi: 10.1002/14651858.CD003669.pub2. PMID: 12917979 Updated.
Similar articles
-
Regional (spinal, epidural, caudal) versus general anaesthesia in preterm infants undergoing inguinal herniorrhaphy in early infancy.Cochrane Database Syst Rev. 2003;(3):CD003669. doi: 10.1002/14651858.CD003669. Cochrane Database Syst Rev. 2003. Update in: Cochrane Database Syst Rev. 2015 Jun 09;(6):CD003669. doi: 10.1002/14651858.CD003669.pub2. PMID: 12917979 Updated.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Effects of targeting lower versus higher arterial oxygen saturations on death or disability in preterm infants.Cochrane Database Syst Rev. 2017 Apr 11;4(4):CD011190. doi: 10.1002/14651858.CD011190.pub2. Cochrane Database Syst Rev. 2017. PMID: 28398697 Free PMC article.
-
Interventions to prevent hypothermia at birth in preterm and/or low birth weight infants.Cochrane Database Syst Rev. 2018 Feb 12;2(2):CD004210. doi: 10.1002/14651858.CD004210.pub5. Cochrane Database Syst Rev. 2018. PMID: 29431872 Free PMC article.
-
Use of biochemical tests of placental function for improving pregnancy outcome.Cochrane Database Syst Rev. 2015 Nov 25;2015(11):CD011202. doi: 10.1002/14651858.CD011202.pub2. Cochrane Database Syst Rev. 2015. PMID: 26602956 Free PMC article.
Cited by
-
Inguinal hernia repair in preterm neonates: is there evidence that spinal or general anaesthesia is the better option regarding intraoperative and postoperative complications? A systematic review and meta-analysis.BMJ Open. 2019 Oct 8;9(10):e028728. doi: 10.1136/bmjopen-2018-028728. BMJ Open. 2019. PMID: 31597647 Free PMC article.
-
[Peribulbar block combined with general anesthesia in babies undergoing laser treatment for retinopathy of prematurity: a retrospective analysis].Braz J Anesthesiol. 2018 Sep-Oct;68(5):431-436. doi: 10.1016/j.bjan.2018.01.004. Epub 2018 Mar 12. Braz J Anesthesiol. 2018. PMID: 29544675 Free PMC article.
-
Regional versus general anaesthesia for improved cognitive function after procedures other than cardiac surgery or neurosurgery in adult and paediatric patients.Cochrane Database Syst Rev. 2016;2016(6):CD008737. doi: 10.1002/14651858.CD008737.pub2. Epub 2016 Jun 22. Cochrane Database Syst Rev. 2016. PMID: 27746701 Free PMC article.
-
Anaesthetic concerns in preterm and term neonates.Indian J Anaesth. 2019 Sep;63(9):771-779. doi: 10.4103/ija.IJA_591_19. Indian J Anaesth. 2019. PMID: 31571691 Free PMC article. Review.
-
Direct bladder hernia after indirect hernia repair in extremely low birth weight babies: two case reports and a review of the literature.J Med Case Rep. 2017 Jan 16;11(1):15. doi: 10.1186/s13256-016-1171-5. J Med Case Rep. 2017. PMID: 28088918 Free PMC article. Review.
References
References to studies included in this review
El‐Gohary 2004 {published data only}
-
- El‐Gohary M, Nabil S, Gamil M, Abdel‐Monem A. Postoperative cardiorespiratory complications in ex‐premature infants: Comparison of general anaesthesia with sevoflurane and awake caudal anaesthesia with ropivacaine. Egyptian Journal of Anesthesia 2004;20(4):391‐7.
Krane 1995 {published data only}
-
- Krane EJ, Haberkern CM, Jacobson LE. Postoperative apnea, bradycardia, and oxygen desaturation in formerly premature infants: prospective comparison of spinal and general anesthesia. Anesthesia and Analgesia 1995;80(1):7‐13. - PubMed
Somri 1998 {published data only}
-
- Somri M, Gaitini L, Vaida S, Collins G, Sabo E, Mogilner G. Postoperative outcome in high‐risk infants undergoing herniorrhaphy: comparison between spinal and general anaesthesia. Anaesthesia 1998;53(8):762‐6. - PubMed
Welborn 1990 {published data only}
-
- Welborn LG, Rice LJ, Hannallah RS, Broadman LM, Ruttiman UE, Fink R. Postoperative apnea in former preterm infants: prospective comparison of spinal and general anesthesia. Anesthesiology 1990;72(5):838‐42. - PubMed
Williams 2001 {published data only}
-
- Williams JM, Stoddart PA, Williams SAR, Wolf AR. Post‐operative recovery after inguinal herniotomy in ex‐premature infants: comparison between sevoflurane and spinal anaesthesia. British Journal of Anaesthesia 2001;86(3):366‐71. - PubMed
References to studies excluded from this review
Somri 2011 {published data only}
-
- Somri M, Coran AG, Mattar I, Teszler C, Shaoul R, Tomkins O, et al. The postoperative occurrence of cardio‐respiratory adverse events in small infants undergoing gastrointestinal surgery: a prospective comparison of general anesthesia and combined spinal‐epidural anesthesia. Pediatric Surgery International 2011;27(11):1173‐8. - PubMed
References to studies awaiting assessment
Das 2005 {published data only}
-
- Das B, Batra Y, Panda N, Rao K. Analgesia in the immediate postoperative period in infants undergoing inguinal herniorrhaphy: A comparison between spinal and general anaesthesia. Journal of Anaesthesiology Clinical Pharmacology 2005;21(2):137‐42.
Kunst 1999 {published data only}
-
- Kunst G, Linderkamp O, Holle R, Motsch J, Martin E. The proportion of high‐risk preterm infants with postoperative apnea and bradycardia is the same after general and spinal anesthesia. The Canadian Journal of Anesthesia 1999;46(1):94‐95. - PubMed
References to ongoing studies
NCT0075660 {published data only}
-
- Davidson A, Sheppard S. A Mulit‐Randomised Controlled Trial Comparing Regional and General Anesthesia for Effects on Neurodevelopmental Outcome and Apnoea in Infants (GAS). ClinicalTrials.gov. http://www.clinicaltrials.gov/ct2/show/NCT00756600 nd. [ISRCTN NCT00756600]
-
- Graaff J, Davidson A, Disma N, Morton N, Whithington D, McCann ME. The GAS study: Success rates practicalities and complications of spinal anaesthesia for neonates and infants. European Journal of Anaesthesiology. Stockholm Sweden, June 2014; Vol. 31:164.
-
- Disma N, Davidson A, Graaff J, Withington D, Morton N, McCann M.E. The GAS study: The postoperative apnea outcome in a RCT comparing spinal and general anaesthesia for infant hernia repair. European Journal of Anaesthesiology. Stockholm, Sweden, June 2014; Vol. 31:2.
Additional references
Berde 2005
-
- Berde CB, Jaksic T, Lynn AM, Maxwell LG, Soriano SG, Tibboel D. Anesthesia and analgesia during and after surgery in neonates. Clinical Therapeutics 2005;27(6):900‐21. [PUBMED: 16117991] - PubMed
Coté 1995
-
- Coté CJ, Zaslavsky A, Downes JJ, Kurth D, Welborn LG, Warner LO, et al. Postoperative apnea in former preterm infants after inguinal herniorrhaphy. A combined analysis. Anesthesiology 1995;82(4):809‐22. [PUBMED: 7717551] - PubMed
DiMaggio 2009
Filan 2012
-
- Filan PM, Hunt RW, Anderson PJ, Doyle LW, Inder TE. Neurologic outcomes in very preterm infants undergoing surgery. The Journal of Pediatrics 2012;160(3):409‐14. [PUBMED: 22048043] - PubMed
Fredriksson 2007
-
- Fredriksson A, Pontén E, Gordh T, Eriksson P. Neonatal exposure to a combination of N‐methyl‐D‐aspartate and gamma‐aminobutyric acid type A receptor anesthetic agents potentiates apoptotic neurodegeneration and persistent behavioral deficits. Anesthesiology 2007;107(3):427‐36. [PUBMED: 17721245] - PubMed
Frumiento 2000
-
- Frumiento C, Abajian JC, Vane DW. Spinal anesthesia for preterm infants undergoing inguinal hernia repair. Archives of Surgery 2000;135(4):445‐51. [PUBMED: 10768710] - PubMed
Georgieff 1986
-
- Georgieff MK, Mills MM, Zempel CE, Chang PN. Catch‐up growth, muscle and fat accretion, and body proportionality of infants one year after newborn intensive care. The Journal of Pediatrics 1989;114(2):288‐92. [PUBMED: 2915289] - PubMed
Geze 2011
-
- Geze S, Imamoğlu M, Cekic B. Awake caudal anesthesia for inguinal hernia operations: successful use in low birth weight neonates. Anaesthesist 2011;60(9):841‐4. [PUBMED: 21755268] - PubMed
Giaufré 1996
-
- Giaufré E, Dalens B, Gombert A. Epidemiology and morbidity of regional anesthesia in children: a one‐year prospective survey of the French‐Language Society of Pediatric Anesthesiologists. Anesthesia & Analgesia 1996;83(5):904‐12. [PUBMED: 8895261] - PubMed
Gollin 1993
-
- Gollin G, Bell C, Dubose R, Touloukian RJ, Seashore JH, Hughes CW, et al. Predictors of postoperative respiratory complications in premature infants after inguinal herniorrhaphy. The Journal of Pediatric Surgery 1993;28(2):244‐7. [PUBMED: 8437090] - PubMed
Grosfeld 1989
-
- Grosfeld JL. Current concepts in inguinal hernia in infants and children. World Journal of Surgery 1989;13(5):506‐15. [PUBMED: 2573200] - PubMed
Hansen 2011
-
- Hansen TG, Pedersen JK, Henneberg SW, Pedersen DA, Murray JC, Morton NS, et al. Academic performance in adolescence after inguinal hernia repair in infancy: a nationwide cohort study. Anesthesiology 2011;114(5):1076‐85. [PUBMED: 21368654] - PubMed
Henderson‐Smart 1995
-
- Henderson‐Smart DJ. Recurrent apnoea. In: Yu VYH editor(s). Bailliere's Clinical Paediatrics. Vol. 3 No. 1 Pulmonary Problems in the Perinatal Period and their Sequelae, London: Bailliere Tindall, 1995:203‐22.
Henderson‐Smart 2001
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook of Interventions for Systematic Reviews Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org. The Cochrane Collaboration.
Jevtovic‐Todorovic 2003
-
- Jevtovic‐Todorovic V, Beals J, Benshoff N, Olney JW. Prolonged exposure to inhalational anesthetic nitrous oxide kills neurons in adult rat brain. Neuroscience 2003;122(3):609‐16. [PUBMED: 14622904] - PubMed
Kumar 2002
-
- Kumar VH, Clive J, Rosenkrantz TS, Bourque MD, Hussain N. Inguinal hernia in preterm infants (< or = 32‐week gestation). Pediatric Surgery International 2002;18(2‐3):147‐52. [PUBMED: 11956782] - PubMed
Kurth 1991
-
- Kurth CD, LeBard SE. Association of postoperative apnea, airway obstruction, and hypoxemia in former premature infants. Anesthesiology 1991;75(1):22‐6. [PUBMED: 2064055] - PubMed
Lee 2011
-
- Lee SL, Gleason JM, Sydorak RM. A critical review of premature infants with inguinal hernias: optimal timing of repair, incarceration risk, and postoperative apnea. Journal of Pediatric Surgery 2011;46(1):217‐20. [PUBMED: 21238671] - PubMed
Liu 1983
-
- Liu LM, Coté CJ, Goudsouzian NG, Ryan JF, Firestone S, Dedrick DF, et al. Life‐threatening apnea in infants recovering from anesthesia. Anesthesiology 1983;59(6):506‐10. [PUBMED: 6650906] - PubMed
Malviya 1993
-
- Malviya S, Swartz J, Lerman J. Are all preterm infants younger than 60 weeks postconceptual age at risk for postanesthetic apnea?. Anesthesiology 1993;78(6):1076‐81. [PUBMED: 8512100] - PubMed
Murphy 2007
-
- Murphy JJ, Swanson T, Ansermino M, Milner R. The frequency of apneas in premature infants after inguinal hernia repair: do they need overnight monitoring in the intensive care unit?. Journal of Pediatric Surgery 2008;43(5):865‐8. [PUBMED: 18485955] - PubMed
NIH 1987
-
- National Institutes of Health. National Institutes of Health Consensus Development Conference on Infantile Apnea and Home Monitoring, Sept 29 to Oct 1, 1986. Pediatrics 1987;79(2):292‐9. [PUBMED: 3808807] - PubMed
Peevy 1986
-
- Peevy KJ, Speed FA, Hoff CJ. Epidemiology of inguinal hernia in preterm neonates. Pediatrics 1986;77:246‐7. [PUBMED: 3753760] - PubMed
Perlman 1985
-
- Perlman JM, Volpe JJ. Episodes of apnea and bradycardia in the preterm newborn: impact on cerebral circulation. Pediatrics 1985;76(3):333‐8. [PUBMED: 4034294] - PubMed
Powell 1986
Rajput 1992
-
- Rajput A, Gauderer MW, Hack M. Inguinal hernias in very low birth weight infants: incidence and timing of repair. Journal of Pediatric Surgery 1992;27(10):1322‐4. [PUBMED: 1403513] - PubMed
Rescorla 1984
-
- Rescorla FJ, Grosfeld JL. Inguinal hernia repair in the perinatal period and early infancy: clinical considerations. Journal of Pediatric Surgery 1984;19:832‐7. [PUBMED: 6520682] - PubMed
RevMan 5.3 [Computer program]
-
- The Nordic Cochrane Centre. The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre. The Cochrane Collaboration, 2014.
Sims 1994
-
- Sims C, Johnson CM. Postoperative apnoea in infants. Anaesthesia and Intensive Care 1994;22(1):40‐5. [PUBMED: 8160948] - PubMed
Tobias 1998
-
- Tobias JD, Burd RS, Helikson MA. Apnea following spinal anaesthesia in two former pre‐term infants. Canadian Journal of Anaesthesia 1998;45(10):985‐9. [PUBMED: 9836035] - PubMed
Welborn 1997
-
- Welborn LG, Greenspun JC. Anesthesia and apnea. Perioperative complications in the former preterm infant. Pediatric Clinics of North America 1994;41(1):181‐98. [MEDLINE: ] - PubMed
References to other published versions of this review
Craven 2003
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous