

Lower Newborn Bone Mineral Content Associated With Maternal Use of Tenofovir Disoproxil Fumarate During Pregnancy
- PMID: 26060285
- PMCID: PMC4551007
- DOI: 10.1093/cid/civ437
Lower Newborn Bone Mineral Content Associated With Maternal Use of Tenofovir Disoproxil Fumarate During Pregnancy
Abstract
Background: Fetal bone effects of maternal tenofovir use have not been well studied. We sought to compare whole-body bone mineral content (BMC) of newborns exposed vs not exposed to tenofovir in utero.
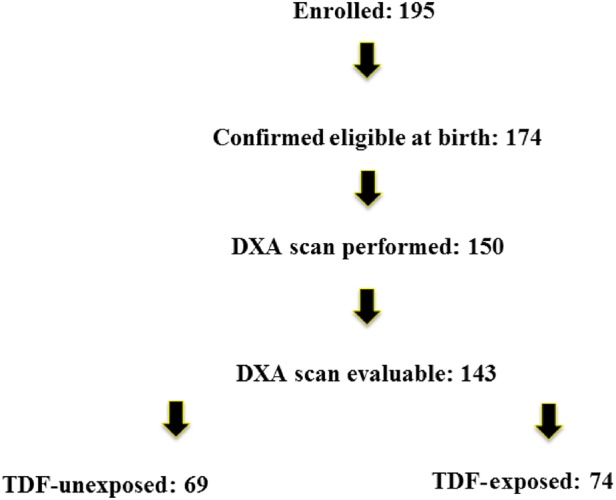
Methods: We enrolled participants from April 2011 to June 2013 at 14 US clinical sites. Singleton infants of women with human immunodeficiency virus (HIV) infection who took tenofovir in late pregnancy (tenofovir-exposed) or no tenofovir during pregnancy (tenofovir-unexposed) were enrolled during late pregnancy or within 72 hours of birth. Infants born before 36 weeks gestation or with confirmed HIV infection were excluded. Whole-body BMC was measured in the first month of life and compared with that of the tenofovir-exposed and tenofovir-unexposed newborns, unadjusted and adjusted for covariates.
Results: Seventy-four tenofovir-exposed and 69 tenofovir-unexposed infants had evaluable BMC measurements. Tenofovir-exposed mothers were more likely to be married (31% vs 22%; P = .04) and to use boosted protease inhibitors (84% vs 62%; P = .004). Tenofovir-exposed newborns did not differ from unexposed newborns on mean gestational age (38.2 vs 38.1 weeks) or mean length (-0.41 vs -0.18) or weight (-0.71 vs -0.48) Z-scores. The mean (standard deviation) BMC of tenofovir-exposed infants was 12% lower than for unexposed infants (56.0 [11.8] vs 63.8 [16.6] g; P = .002). The adjusted mean bone mineral content was 5.3 g lower (95% confidence interval, -9.5, -1.2; P = .013) in the tenofovir-exposed infants.
Conclusions: Maternal tenofovir use is associated with significantly lower neonatal BMC. The duration and clinical significance of this finding should be evaluated in longitudinal studies.
Clinical trials registration: ClinicalTrials.gov NCT01310023.
Keywords: HIV; infant bone mineral content; intrauterine exposure; tenofovir.
Published by Oxford University Press on behalf of the Infectious Diseases Society of America 2015. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
Comment in
-
Reply to Koo et al.Clin Infect Dis. 2016 May 15;62(10):1324-5. doi: 10.1093/cid/ciw116. Epub 2016 Mar 1. Clin Infect Dis. 2016. PMID: 26936672 Free PMC article. No abstract available.
-
Bone Mineral Content in Neonates.Clin Infect Dis. 2016 May 15;62(10):1323-4. doi: 10.1093/cid/ciw115. Epub 2016 Mar 1. Clin Infect Dis. 2016. PMID: 26936674 No abstract available.
References
-
- World Health Organization consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach, 2013. Available at: http://www.who.int/hiv/pub/guidelines/arv2013/download/en/. Accessed 15 March 2015. - PubMed
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services; Available at: http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed 15 March 2015.
-
- Gallant JE, Staszewski S, Pozniak AL et al. . Efficacy and safety of tenofovir DF vs stavudine in combination therapy in antiretroviral-naive patients: a 3-year randomized trial. JAMA 2004; 292:191–201. - PubMed
-
- Stellbrink H-J, Orkin C, Arribas JR et al. . Comparison of changes in bone density and turnover with abacavir-lamivudine versus tenofovir-emtricitabine in HIV-infected adults: 48-week results from the ASSERT study . Clin Infect Dis 2010; 51:963–72. - PubMed
-
- McComsey GA, Kitch D, Daar ES et al. . Bone mineral density and fractures in antiretroviral-naive persons randomized to receive abacavir-lamivudine or tenofovir disoproxil fumarate-emtricitabine along with efavirenz or atazanavir-ritonavir: AIDS Clinical Trials Group A5224s, a Substudy of ACTG A5202. J Infect Dis 2011; 203:1791–801. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
