

Prioritising Infectious Disease Mapping
- PMID: 26061527
- PMCID: PMC4464526
- DOI: 10.1371/journal.pntd.0003756
Prioritising Infectious Disease Mapping
Abstract
Background: Increasing volumes of data and computational capacity afford unprecedented opportunities to scale up infectious disease (ID) mapping for public health uses. Whilst a large number of IDs show global spatial variation, comprehensive knowledge of these geographic patterns is poor. Here we use an objective method to prioritise mapping efforts to begin to address the large deficit in global disease maps currently available.
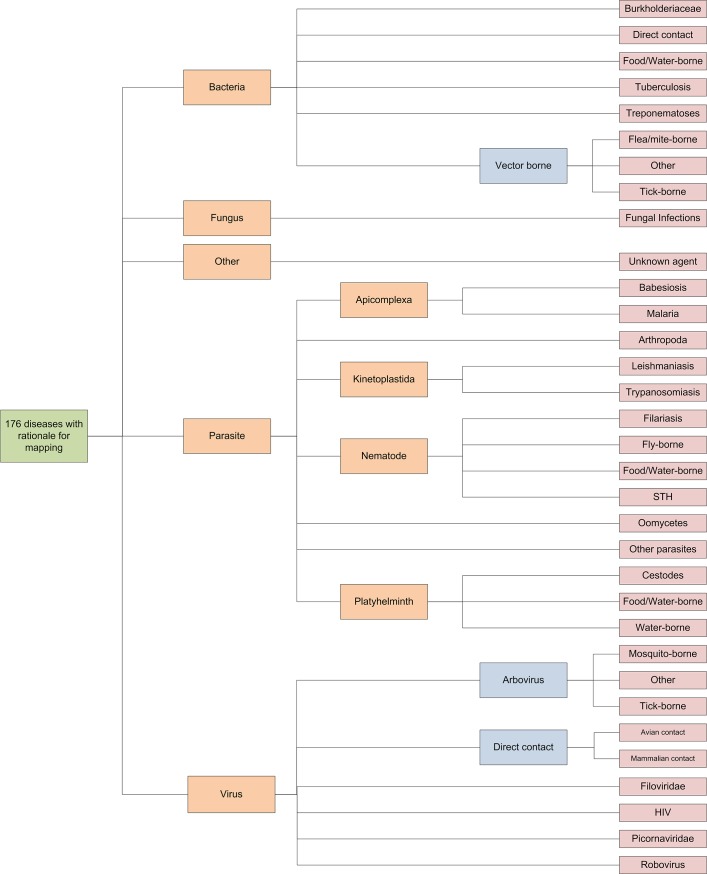
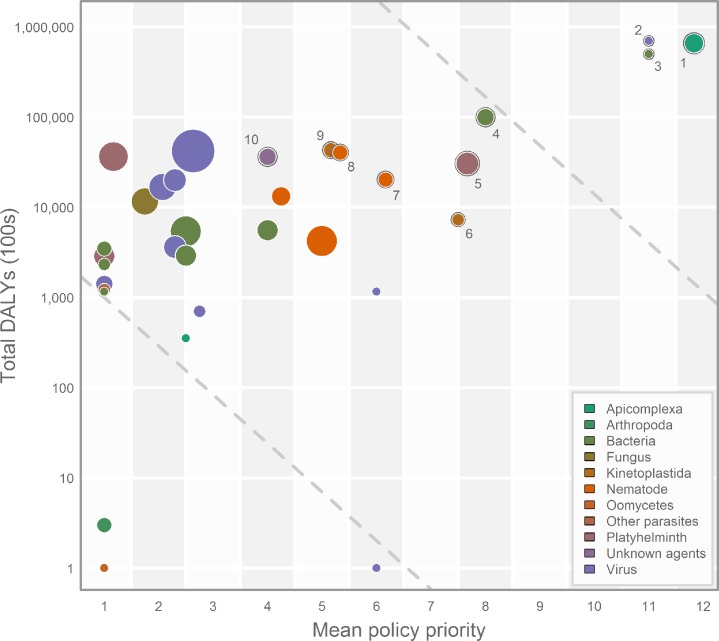
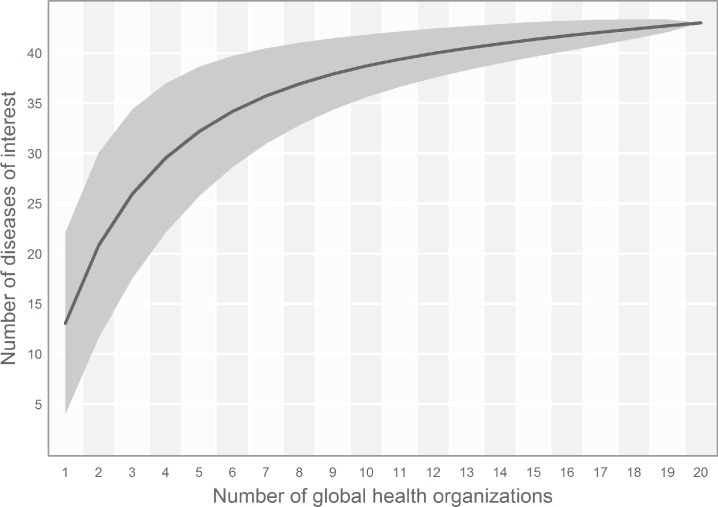
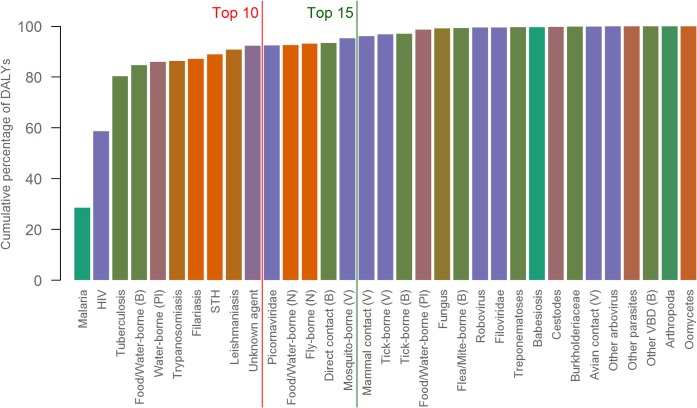
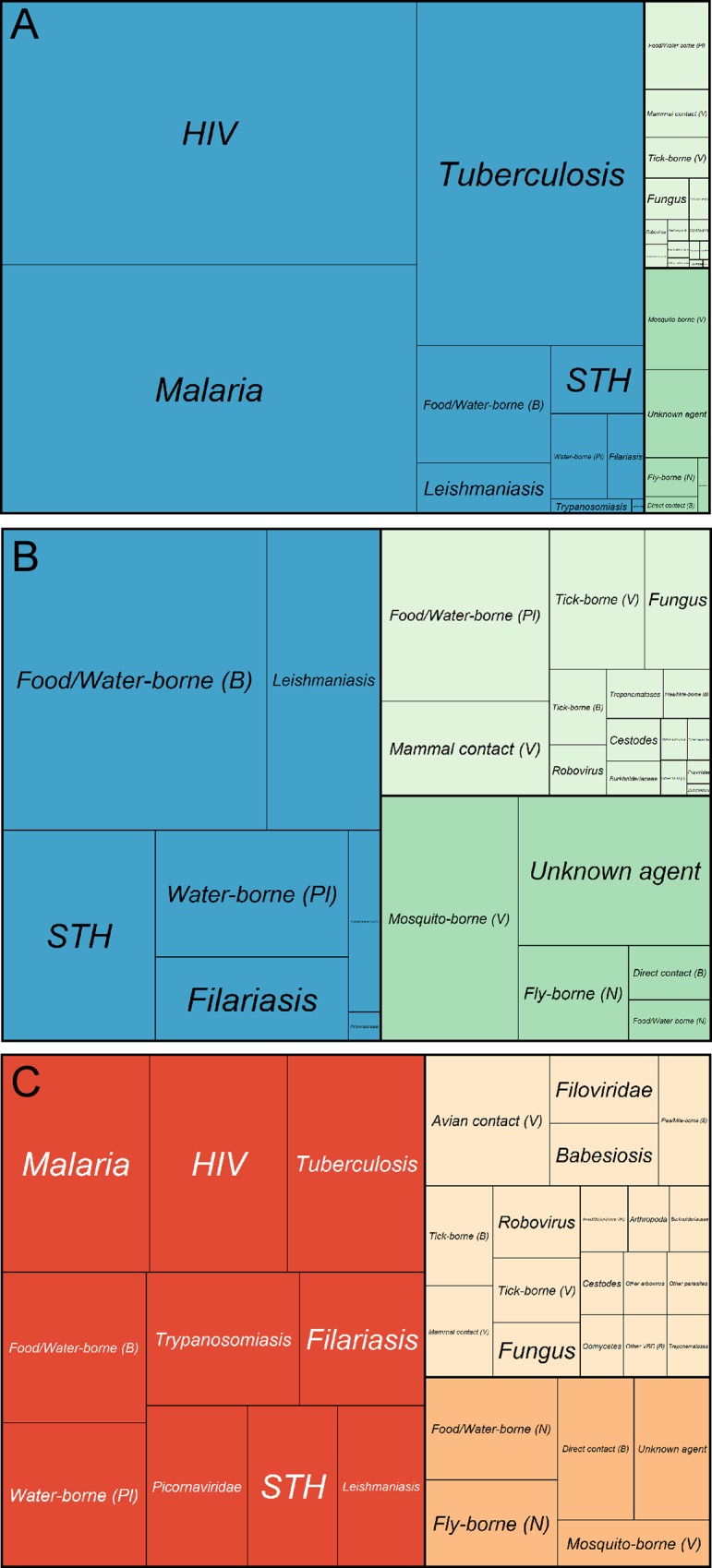
Methodology/principal findings: Automation of ID mapping requires bespoke methodological adjustments tailored to the epidemiological characteristics of different types of diseases. Diseases were therefore grouped into 33 clusters based upon taxonomic divisions and shared epidemiological characteristics. Disability-adjusted life years, derived from the Global Burden of Disease 2013 study, were used as a globally consistent metric of disease burden. A review of global health stakeholders, existing literature and national health priorities was undertaken to assess relative interest in the diseases. The clusters were ranked by combining both metrics, which identified 44 diseases of main concern within 15 principle clusters. Whilst malaria, HIV and tuberculosis were the highest priority due to their considerable burden, the high priority clusters were dominated by neglected tropical diseases and vector-borne parasites.
Conclusions/significance: A quantitative, easily-updated and flexible framework for prioritising diseases is presented here. The study identifies a possible future strategy for those diseases where significant knowledge gaps remain, as well as recognising those where global mapping programs have already made significant progress. For many conditions, potential shared epidemiological information has yet to be exploited.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: SJB is a deputy editor of PLoS Neglected Tropical Diseases.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
