

The prognostic role of HER2 expression in ductal breast carcinoma in situ (DCIS); a population-based cohort study
- PMID: 26062614
- PMCID: PMC4464713
- DOI: 10.1186/s12885-015-1479-3
The prognostic role of HER2 expression in ductal breast carcinoma in situ (DCIS); a population-based cohort study
Abstract
Background: HER2 is a well-established prognostic and predictive factor in invasive breast cancer. The role of HER2 in ductal breast carcinoma in situ (DCIS) is debated and recent data have suggested that HER2 is mainly related to in situ recurrences. Our aim was to study HER2 as a prognostic factor in a large population based cohort of DCIS with long-term follow-up.
Methods: All 458 patients diagnosed with a primary DCIS 1986-2004 in two Swedish counties were included. Silver-enhanced in situ hybridisation (SISH) was used for detection of HER2 gene amplification and protein expression was assessed by immunohistochemistry (IHC) in tissue microarrays. HER2 positivity was defined as amplified HER2 gene and/or HER2 3+ by IHC. HER2 status in relation to new ipsilateral events (IBE) and Invasive Breast Cancer Recurrences, local or distant (IBCR) was assessed by Kaplan-Meier survival analyses and Cox proportional hazards regression models.
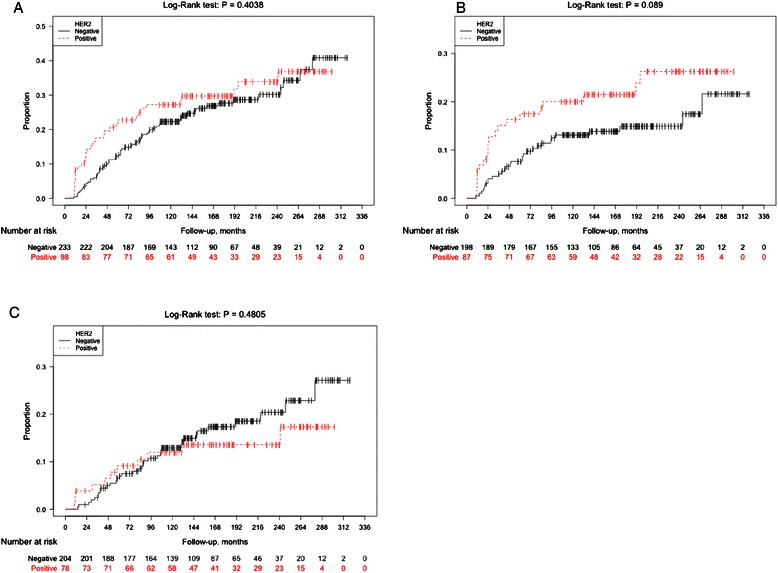
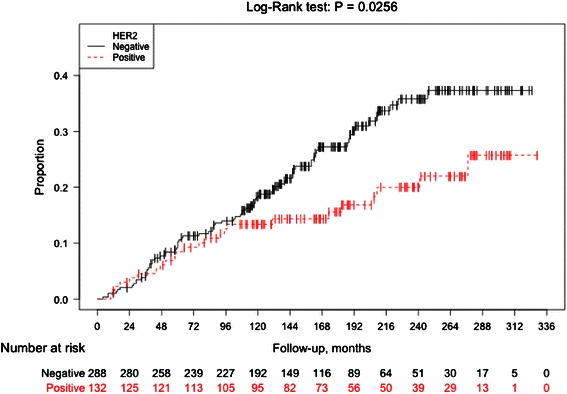
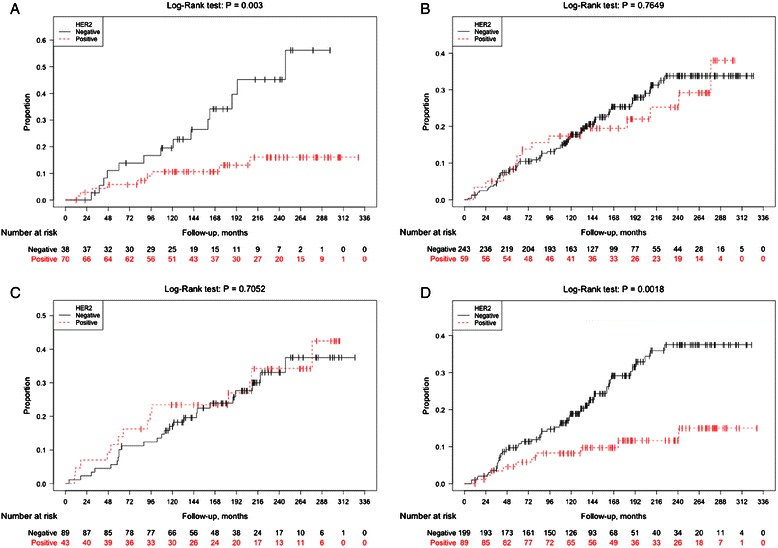
Results: Primary DCIS was screening-detected in 75.5% of cases. Breast conserving surgery (BCS) was performed in 78.6% of whom 44.0% received postoperative radiotherapy. No patients received adjuvant endocrine- or chemotherapy. The majority of DCIS could be HER2 classified (N=420 (91.7%)); 132 HER2 positive (31%) and 288 HER2 negative (69%)). HER2 positivity was related to large tumor size (P=0.002), high grade (P<0.001) and ER- and PR negativity (P<0.001 for both). During follow-up (mean 184 months), 106 IBCRs and 105 IBEs were identified among all 458 cases corresponding to 54 in situ and 51 invasive recurrences. Eighteen women died from breast cancer and another 114 had died from other causes. The risk of IBCR was statistically significantly lower subsequent to a HER2 positive DCIS compared to a HER2 negative DCIS, (Log-Rank P=0.03, (HR) 0.60 (95% CI 0.38-0.94)). Remarkably, the curves did not separate until after 10 years. In ER-stratified analyses, HER2 positive DCIS was associated with lower risk of IBCR among women with ER negative DCIS (Log-Rank P=0.003), but not for women with ER positive DCIS.
Conclusions: Improved prognostic tools for DCIS patients are warranted to tailor adjuvant therapy. Here, we demonstrate that HER2 positive disease in the primary DCIS is associated with lower risk of recurrent invasive breast cancer.
Figures
References
-
- Lee LA, Silverstein MJ, Chung CT, Macdonald H, Sanghavi P, Epstein M, Holmes DR, Silberman H, Ye W, Lagios MD. Breast cancer-specific mortality after invasive local recurrence in patients with ductal carcinoma-in-situ of the breast. Am J Surg. 2006;192:416–9. doi: 10.1016/j.amjsurg.2006.06.005. - DOI - PubMed
-
- Ringberg A, Nordgren H, Thorstensson S, Idvall I, Garmo H, Granstrand B, Arnesson LG, Sandelin K, Wallgren A, Anderson H, et al. Histopathological risk factors for ipsilateral breast events after breast conserving treatment for ductal carcinoma in situ of the breast–results from the Swedish randomised trial. Eur J Cancer. 2007;43:291–8. doi: 10.1016/j.ejca.2006.09.018. - DOI - PubMed
-
- Yi M, Meric-Bernstam F, Kuerer HM, Mittendorf EA, Bedrosian I, Lucci A, Hwang RF, Crow JR, Luo S, Hunt KK. Evaluation of a breast cancer nomogram for predicting risk of ipsilateral breast tumor recurrences in patients with ductal carcinoma in situ after local excision. J Clin Oncol. 2012;30:600–7. doi: 10.1200/JCO.2011.36.4976. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
