

A Mobile Health Intervention Supporting Heart Failure Patients and Their Informal Caregivers: A Randomized Comparative Effectiveness Trial
- PMID: 26063161
- PMCID: PMC4526929
- DOI: 10.2196/jmir.4550
A Mobile Health Intervention Supporting Heart Failure Patients and Their Informal Caregivers: A Randomized Comparative Effectiveness Trial
Abstract
Background: Mobile health (mHealth) interventions may improve heart failure (HF) self-care, but standard models do not address informal caregivers' needs for information about the patient's status or how the caregiver can help.
Objective: We evaluated mHealth support for caregivers of HF patients over and above the impact of a standard mHealth approach.
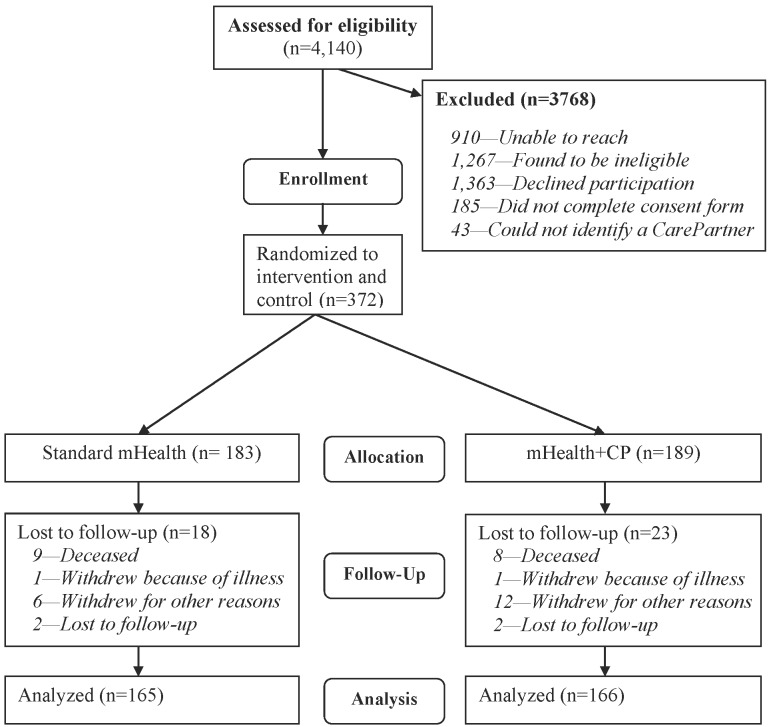
Methods: We identified 331 HF patients from Department of Veterans Affairs outpatient clinics. All patients identified a "CarePartner" outside their household. Patients randomized to "standard mHealth" (n=165) received 12 months of weekly interactive voice response (IVR) calls including questions about their health and self-management. Based on patients' responses, they received tailored self-management advice, and their clinical team received structured fax alerts regarding serious health concerns. Patients randomized to "mHealth+CP" (n=166) received an identical intervention, but with automated emails sent to their CarePartner after each IVR call, including feedback about the patient's status and suggestions for how the CarePartner could support disease care. Self-care and symptoms were measured via 6- and 12-month telephone surveys with a research associate. Self-care and symptom data also were collected through the weekly IVR assessments.
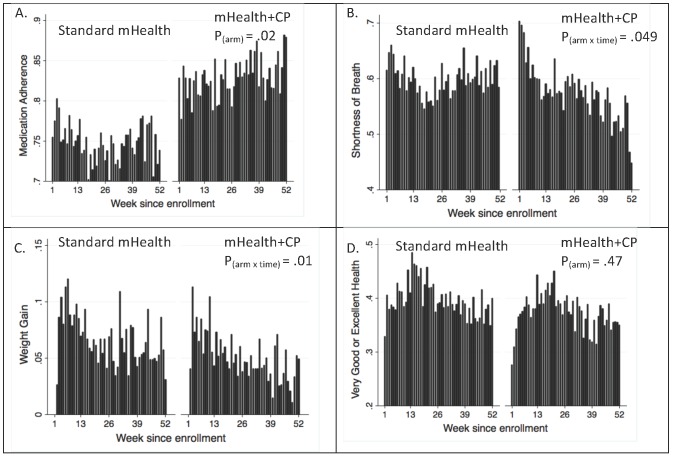
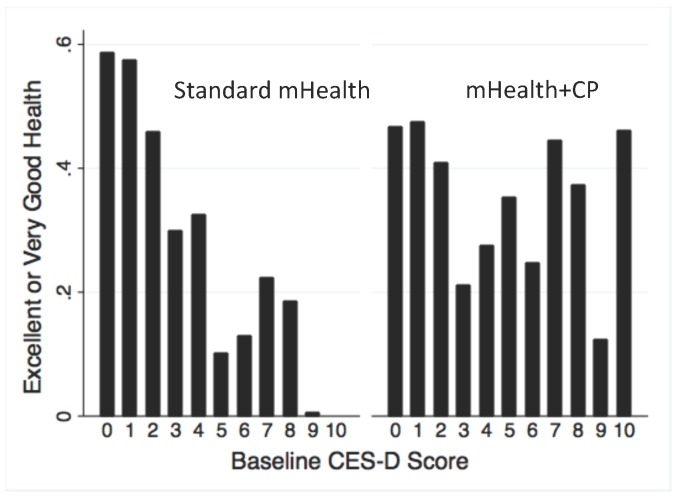
Results: Participants were on average 67.8 years of age, 99% were male (329/331), 77% where white (255/331), and 59% were married (195/331). During 15,709 call-weeks of attempted IVR assessments, patients completed 90% of their calls with no difference in completion rates between arms. At both endpoints, composite quality of life scores were similar across arms. However, more mHealth+CP patients reported taking medications as prescribed at 6 months (8.8% more, 95% CI 1.2-16.5, P=.02) and 12 months (13.8% more, CI 3.7-23.8, P<.01), and 10.2% more mHealth+CP patients reported talking with their CarePartner at least twice per week at the 6-month follow-up (P=.048). mHealth+CP patients were less likely to report negative emotions during those interactions at both endpoints (both P<.05), were consistently more likely to report taking medications as prescribed during weekly IVR assessments, and also were less likely to report breathing problems or weight gains (all P<.05). Among patients with more depressive symptoms at enrollment, those randomized to mHealth+CP were more likely than standard mHealth patients to report excellent or very good general health during weekly IVR calls.
Conclusions: Compared to a relatively intensive model of IVR monitoring, self-management assistance, and clinician alerts, a model including automated feedback to an informal caregiver outside the household improved HF patients' medication adherence and caregiver communication. mHealth+CP may also decrease patients' risk of HF exacerbations related to shortness of breath and sudden weight gains. mHealth+CP may improve quality of life among patients with greater depressive symptoms. Weekly health and self-care monitoring via mHealth tools may identify intervention effects in mHealth trials that go undetected using typical, infrequent retrospective surveys.
Trial registration: ClinicalTrials.gov NCT00555360; https://clinicaltrials.gov/ct2/show/NCT00555360 (Archived by WebCite at http://www.webcitation.org/6Z4Tsk78B).
Keywords: disease management; heart failure; mobile health; self-management; telehealth.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures


References
-
- Harrison Margaret B, Browne Gina B, Roberts Jacqueline, Tugwell Peter, Gafni Amiram, Graham Ian D. Quality of life of individuals with heart failure: a randomized trial of the effectiveness of two models of hospital-to-home transition. Med Care. 2002 Apr;40(4):271–82. - PubMed
-
- Benatar Daniel, Bondmass Mary, Ghitelman Jaime, Avitall Boaz. Outcomes of chronic heart failure. Arch Intern Med. 2003 Feb 10;163(3):347–52.ioi10871 - PubMed
-
- Artinian Nancy T, Magnan Morris, Sloan Michelle, Lange M Patricia. Self-care behaviors among patients with heart failure. Heart Lung. 2002;31(3):161–72.S0147956302059812 - PubMed
-
- Ni H, Nauman D, Burgess D, Wise K, Crispell K, Hershberger R E. Factors influencing knowledge of and adherence to self-care among patients with heart failure. Arch Intern Med. 1999 Jul 26;159(14):1613–9. - PubMed
-
- Heidenreich Paul A, Trogdon Justin G, Khavjou Olga A, Butler Javed, Dracup Kathleen, Ezekowitz Michael D, Finkelstein Eric Andrew, Hong Yuling, Johnston S Claiborne, Khera Amit, Lloyd-Jones Donald M, Nelson Sue A, Nichol Graham, Orenstein Diane, Wilson Peter W F, Woo Y Joseph, American Heart Association Advocacy Coordinating Committee. Stroke Council. Council on Cardiovascular Radiology and Intervention. Council on Clinical Cardiology. Council on Epidemiology and Prevention. Council on Arteriosclerosis. Thrombosis and Vascular Biology. Council on Cardiopulmonary. Critical Care. Perioperative and Resuscitation. Council on Cardiovascular Nursing. Council on the Kidney in Cardiovascular Disease. Council on Cardiovascular Surgery and Anesthesia‚ Interdisciplinary Council on Quality of Care and Outcomes Research Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011 Mar 1;123(8):933–44. doi: 10.1161/CIR.0b013e31820a55f5. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=21262990 CIR.0b013e31820a55f5 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
