

New horizons for newborn brain protection: enhancing endogenous neuroprotection
- PMID: 26063194
- PMCID: PMC4680177
- DOI: 10.1136/archdischild-2014-306284
New horizons for newborn brain protection: enhancing endogenous neuroprotection
Abstract
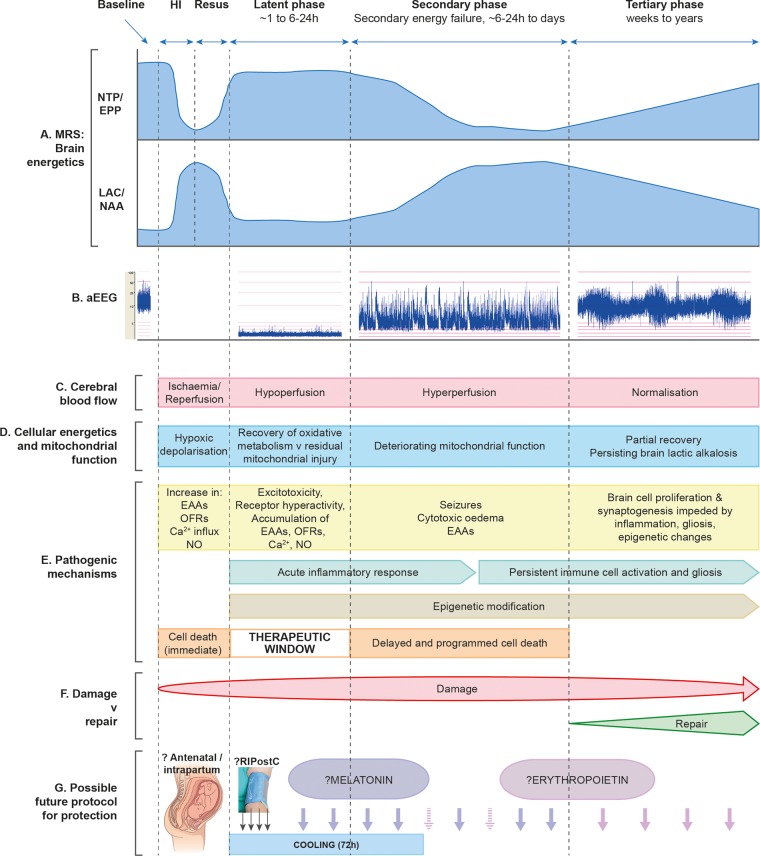
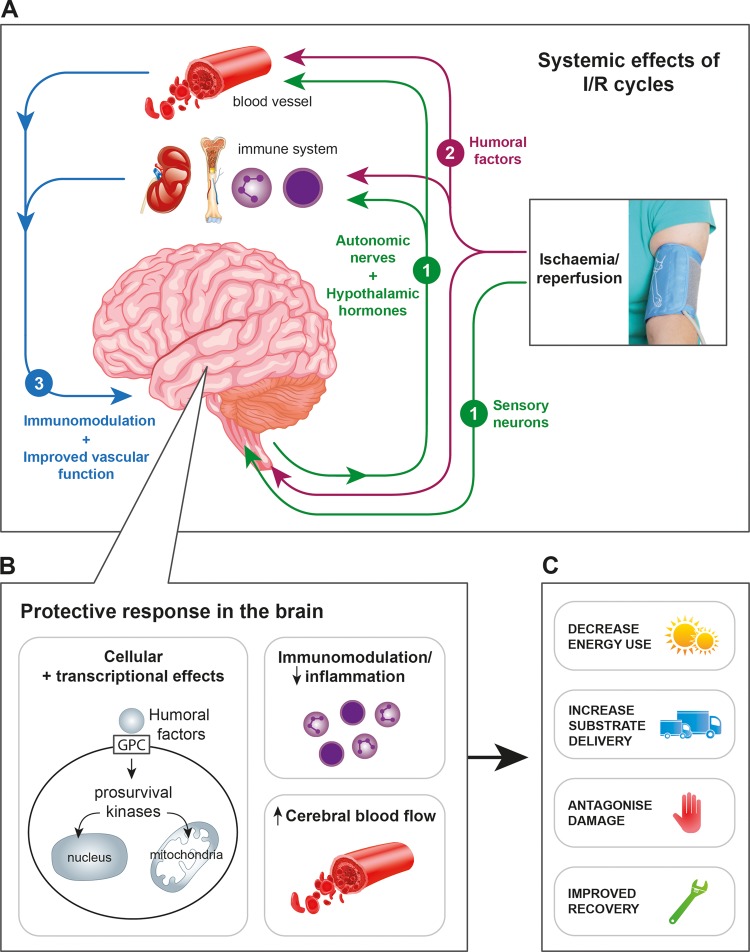
Intrapartum-related events are the third leading cause of childhood mortality worldwide and result in one million neurodisabled survivors each year. Infants exposed to a perinatal insult typically present with neonatal encephalopathy (NE). The contribution of pure hypoxia-ischaemia (HI) to NE has been debated; over the last decade, the sensitising effect of inflammation in the aetiology of NE and neurodisability is recognised. Therapeutic hypothermia is standard care for NE in high-income countries; however, its benefit in encephalopathic babies with sepsis or in those born following chorioamnionitis is unclear. It is now recognised that the phases of brain injury extend into a tertiary phase, which lasts for weeks to years after the initial insult and opens up new possibilities for therapy.There has been a recent focus on understanding endogenous neuroprotection and how to boost it or to supplement its effectors therapeutically once damage to the brain has occurred as in NE. In this review, we focus on strategies that can augment the body's own endogenous neuroprotection. We discuss in particular remote ischaemic postconditioning whereby endogenous brain tolerance can be activated through hypoxia/reperfusion stimuli started immediately after the index hypoxic-ischaemic insult. Therapeutic hypothermia, melatonin, erythropoietin and cannabinoids are examples of ways we can supplement the endogenous response to HI to obtain its full neuroprotective potential. Achieving the correct balance of interventions at the correct time in relation to the nature and stage of injury will be a significant challenge in the next decade.
Keywords: Birth asphyxia; Melatonin; Neonatal encephalopathy; Neuroprotection; Post Conditioning.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical