

Estrogen Receptor Status and the Future Burden of Invasive and In Situ Breast Cancers in the United States
- PMID: 26063794
- PMCID: PMC4836802
- DOI: 10.1093/jnci/djv159
Estrogen Receptor Status and the Future Burden of Invasive and In Situ Breast Cancers in the United States
Abstract
Background: No study has predicted the future incidence rate and annual burden (number) of new cases in the United States of invasive and in situ female breast cancers stratified by the estrogen receptor (ER) status.
Methods: We constructed forecasts for women age 30 to 84 years in 2011 through 2030 using cancer incidence data from the Surveillance, Epidemiology, and End Results Program, novel age-period-cohort forecasting models, and population projections from the US Census Bureau.
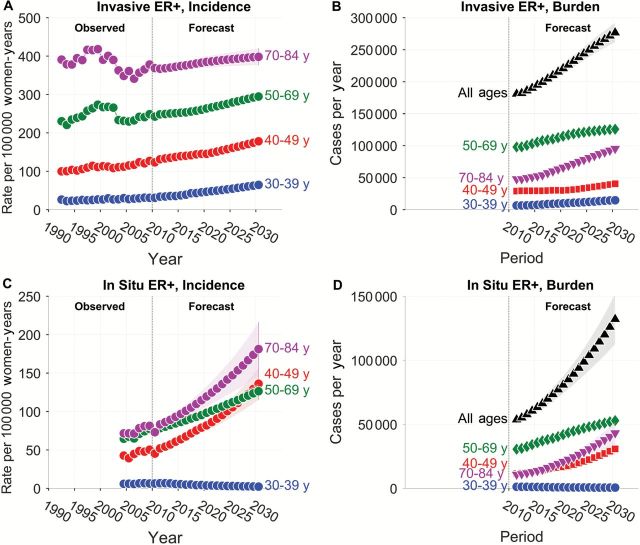
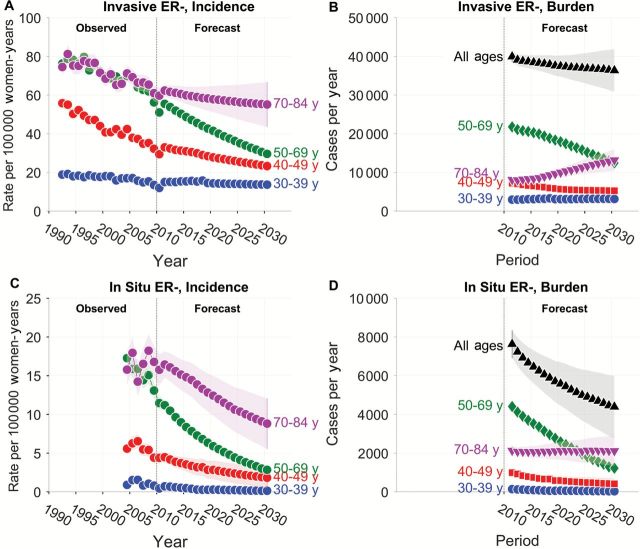
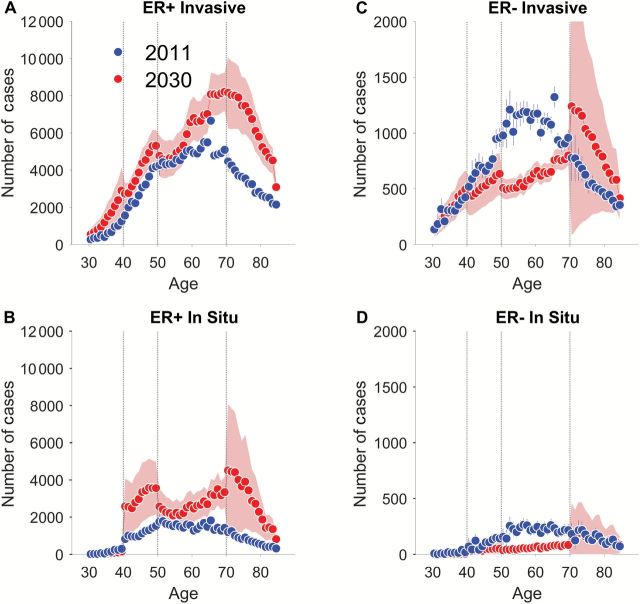
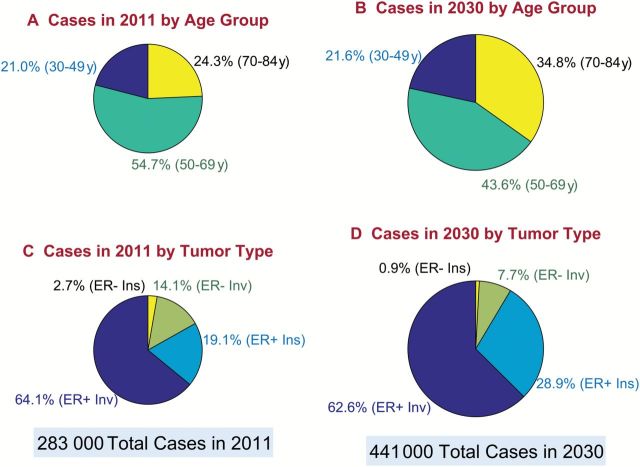
Results: The total number of new tumors (invasive plus in situ) is expected to rise from 283 000 in 2011 to 441 000 in 2030 (plausible range 353 500 to 466 700 cases). The proportion of all new case patients age 70 to 84 years is expected to increase from 24.3% to 34.8%, while the proportion ages 50 to 69 years is expected to decrease from 54.7% to 43.6%. The proportion of ER-positive invasive cancers is expected to remain nearly the same at 62.6%, whereas the proportion of ER-positive in situ cancers is expected to increase from 19.1% to 28.9%. The proportion of ER-negative cancers (invasive and in situ) is expected to decrease from 16.8% to 8.6%.
Conclusions: Breast cancer overall will rise in the United States through 2030, especially for ER-positive in situ tumors among women age 70 to 84 years. In contrast, ER-negative invasive and in situ tumors will fall, for reasons that are not fully understood. These results highlight a need to optimize case management among older women, characterize the natural history of in situ cancers, and identify those factors responsible for declining ER-negative incidence.
Published by Oxford University Press 2015. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
References
-
- Institute NC. Breast Cancer Risk in American Women. National Cancer Institute; 2014. Available at: http://www.cancer.gov/cancertopics/factsheet/detection/probability-breas.... Accessed Jan 6, 2015.
-
- Smith BD, Smith GL, Hurria A, Hortobagyi GN, Buchholz TA. Future of cancer incidence in the United States: burdens upon an aging, changing nation. J Clin Oncol. 2009;27(17):2758–2765. - PubMed
-
- Althuis MD, Fergenbaum JH, Garcia-Closas M, Brinton LA, Madigan MP, Sherman ME. Etiology of hormone receptor-defined breast cancer: a systematic review of the literature. Cancer Epidemiol Biomarkers Prev. 2004;13(10):1558–1568. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
