

Trends in pediatric pulmonary hypertension-related hospitalizations in the United States from 2000-2009
- PMID: 26064460
- PMCID: PMC4449246
- DOI: 10.1086/681226
Trends in pediatric pulmonary hypertension-related hospitalizations in the United States from 2000-2009
Abstract
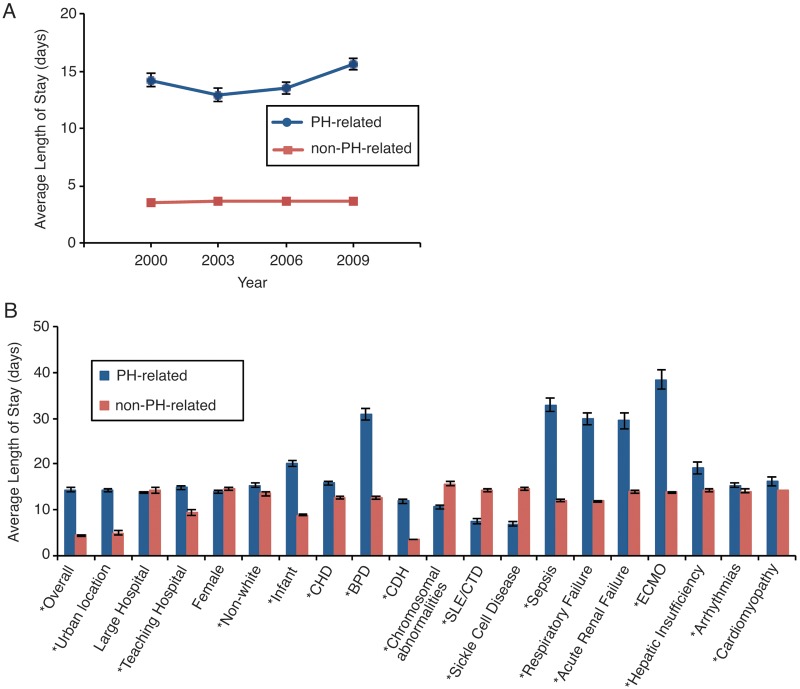
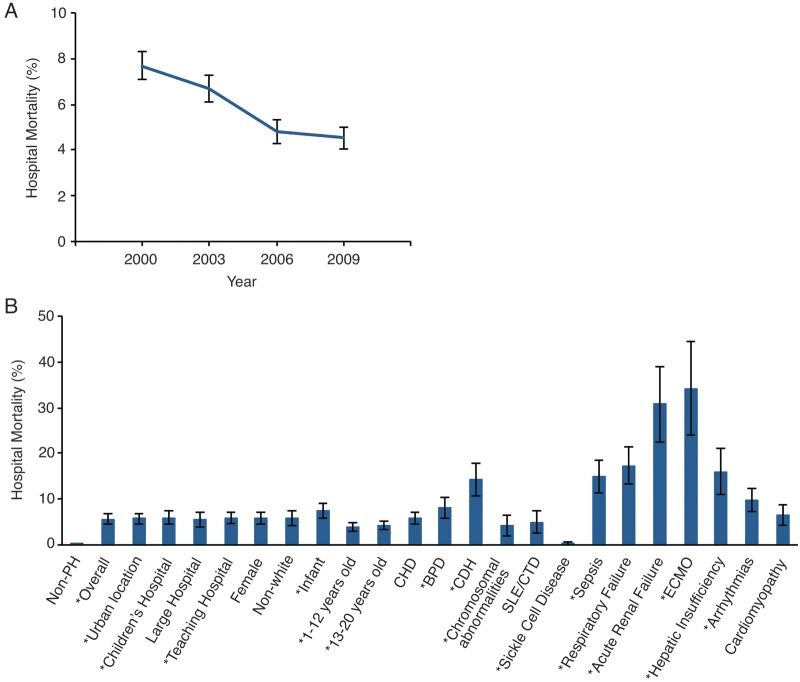
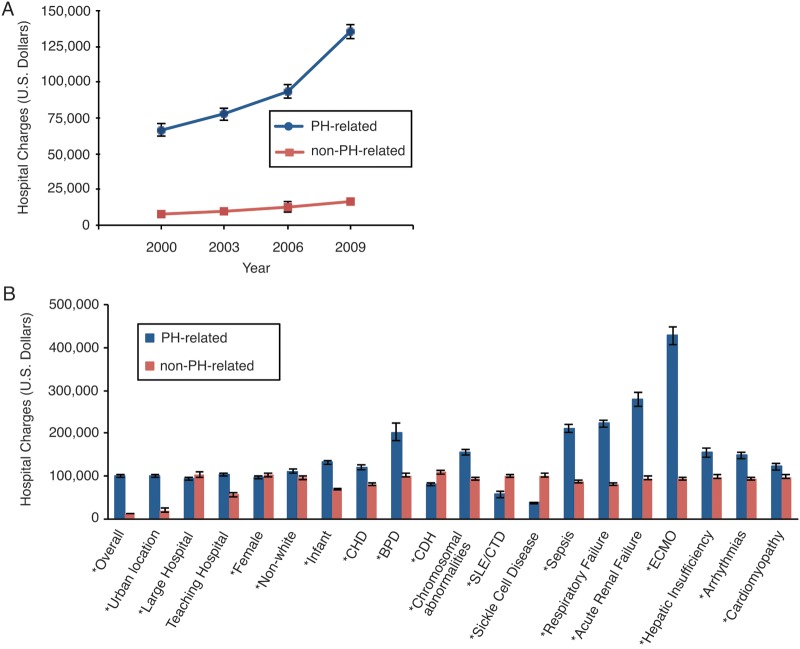
There are few data on the epidemiology of pulmonary hypertension (PH)-related hospitalizations in children in the United States. Our aim was to determine hospital mortality, length of hospitalization, and hospital charges pertaining to PH-related hospitalizations and also the effects of codiagnoses and comorbidities. A retrospective review of the Kids' Inpatient Database during the years 2000, 2003, 2006, and 2009 was analyzed for patients ≤20 years of age with a diagnosis of PH by ICD-9 (International Classification of Diseases, Ninth Revision) codes, along with associated diagnoses and comorbidities. Descriptive statistics, including Rao-Scott χ(2), ANOVA, and logistic regression models, were utilized on weighted values with survey analysis procedures. The number of PH-related hospital admissions is rising, from an estimated 7,331 (95% confidence interval [CI]: 5,556-9,106) in 2000 to 10,792 (95% CI: 8,568-13,016) in 2009. While infant age and congenital heart disease were most commonly associated with PH-related hospitalizations, they were not associated with mortality. Overall mortality for PH-related hospitalizations was greater than that for hospitalizations not associated with PH, 5.7% versus 0.4% (odds ratio: 16.22 [95% CI: 14.78%-17.8%], P < 0.001), but mortality is decreasing over time. Sepsis, respiratory failure, acute renal failure, hepatic insufficiency, arrhythmias, and the use of extracorporeal membrane oxygenation are associated with mortality. The number of PH-related hospitalizations is increasing in the United States. The demographics of PH in this study are evolving. Despite the increasing prevalence, mortality is improving.
Keywords: epidemiology; pediatrics; pulmonary hypertension; survival.
Figures
References
-
- Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, Gomez Sanchez MA, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2013;62(25 suppl.):D34–D41. - PubMed
-
- Barst RJ, McGoon MD, Elliott CG, Foreman AJ, Miller DP, Ivy DD. Survival in childhood pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management. Circulation 2012;125(1):113–122. - PubMed
-
- Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiéry JL, Barbera JA, Beghetti M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J 2009;30(20):2493–2537. - PubMed
-
- Fraisse A, Jaïs X, Schleich JM, Filippo S, Maragnès P, Beghetti M, Gressin V, et al. Characteristics and prospective 2-year follow-up of children with pulmonary arterial hypertension in France. Arch Cardiovasc Dis 2010;103(2):66–74. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
