

Review
doi: 10.1155/2015/697010.
Epub 2015 Apr 30.
Diabetic Kidney Disease: Pathophysiology and Therapeutic Targets
Affiliations
- PMID: 26064987
- PMCID: PMC4430644
- DOI: 10.1155/2015/697010
Item in Clipboard
Review
Diabetic Kidney Disease: Pathophysiology and Therapeutic Targets
J Diabetes Res.
2015.
Abstract
Diabetes is a worldwide epidemic that has led to a rise in diabetic kidney disease (DKD). Over the past two decades, there has been significant clarification of the various pathways implicated in the pathogenesis of DKD. Nonetheless, very little has changed in the way clinicians manage patients with this disorder. Indeed, treatment is primarily centered on controlling hyperglycemia and hypertension and inhibiting the renin-angiotensin system. The purpose of this review is to describe the current understanding of how the hemodynamic, metabolic, inflammatory, and alternative pathways are all entangled in pathogenesis of DKD and detail the various therapeutic targets that may one day play a role in quelling this epidemic.
Figures
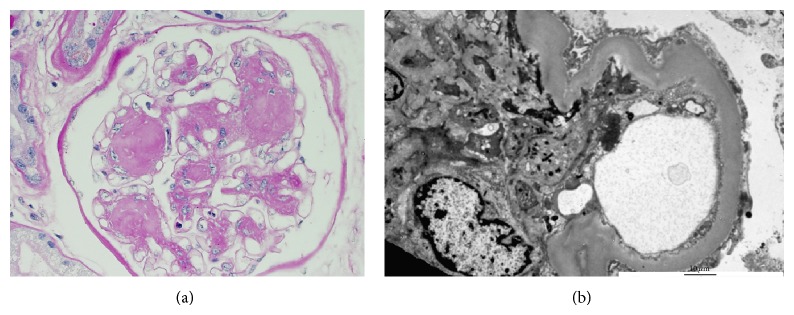
(a) Light microscopy with hematoxylin-eosin staining reveals extensive mesangial expansion without marked increase in cellularity. A Kimmelstiel-Wilson (KW) lesion is shown here and refers to the nodular glomerulosclerosis that can be seen in late disease but is not as common as diffuse diabetic glomerulosclerosis. KW lesions are usually spherical and eosinophilic and have a central hypocellular or acellular area. Mesangial expansion and KW lesions are both due to increased extracellular matrix production. (b) Electron microscopy reveals a thickened basement membrane and podocyte foot process effacement.
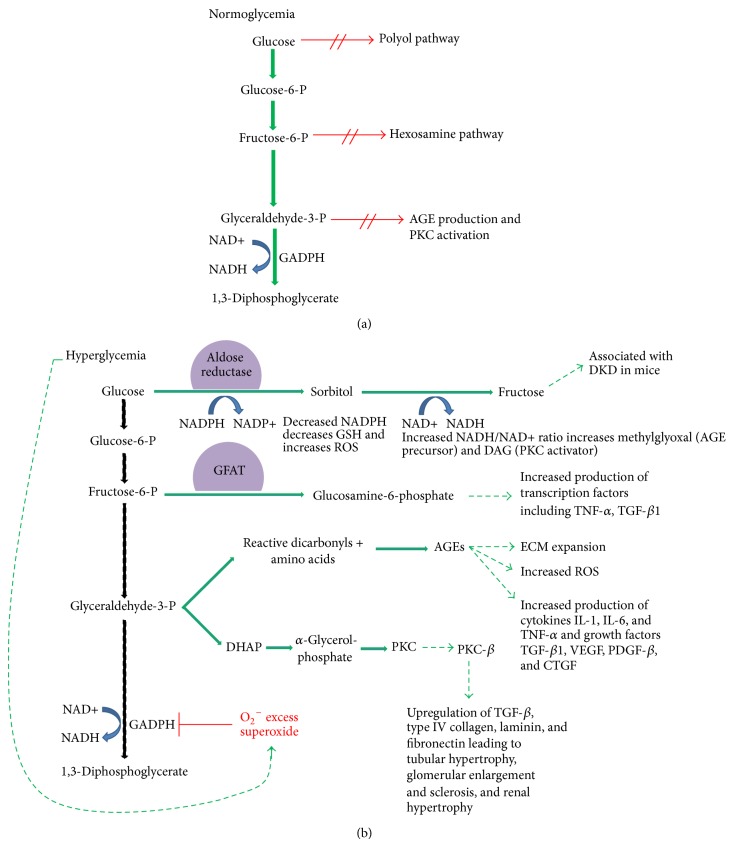
(a) Glycolysis is the biochemical pathway in which glucose is broken down by cells to make energy. In a normoglycemic environment, that is, in patients without diabetes, glycolysis proceeds down its well described path without shunting into the polyol pathway, hexosamine pathway, or pathways that would lead to AGE production or PKC activation. (b) In a hyperglycemic environment, as would be seen in patients with either type 1 or type 2 diabetes, high glucose conditions lead to activation of excess superoxide which then inhibits the enzyme GADPH. This prevents glycolysis from proceeding down its natural course and creates a backlog of glycolysis precursors. Increased levels of glucose upregulate the polyol pathway whereas increased levels of fructose-6-phosphate upregulate the hexosamine pathway. Increased levels of glyceraldehyde-3-phosphate upregulate both AGE precursors and DAG, the latter being a cofactor for PKC activation.
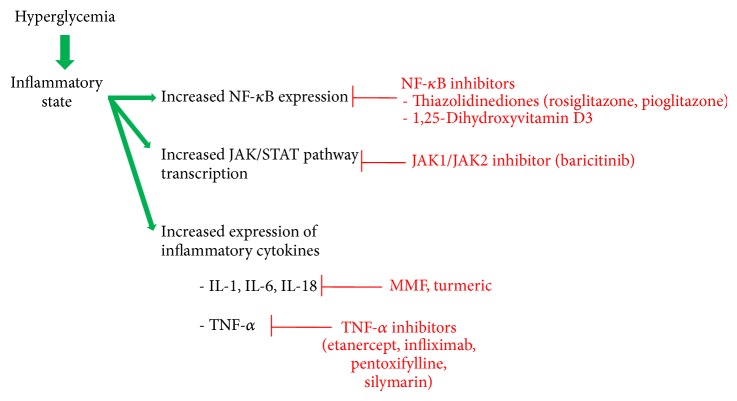
A schematic summary of the therapeutics that have been identified in the inflammatory pathway. The inflammatory state occurs as a result of hyperglycemia and is seen in patients with both type 1 and 2 diabetes.
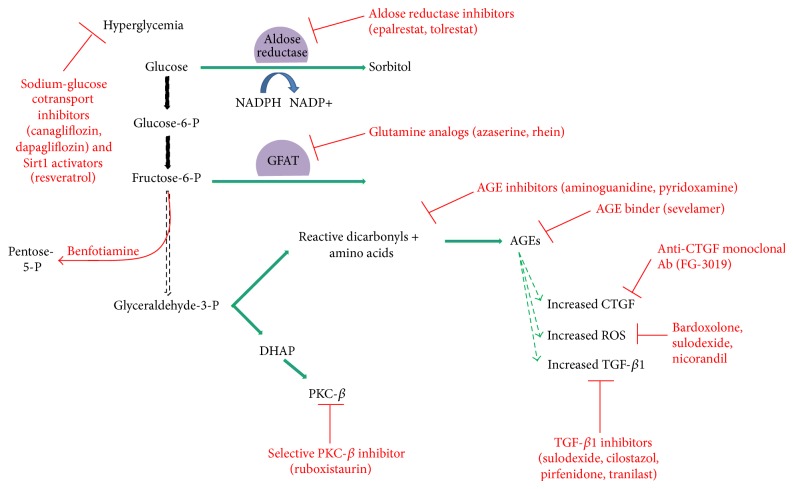
A schematic summary of the various therapeutic agents that have been identified in the metabolic and alternative pathways is shown below. As noted in Figure 2(b), a hyperglycemic milieu shunts glucose metabolism away from the classic glycolysis pathway as is typically seen in patients with type 1 and type 2 diabetes. Sodium-glucose cotransport (SLGT2) inhibitors and Sirt1 activators play a role in alternative pathway and are noted in the upper left. SLGT2 inhibitors combat hyperglycemia by inducing glucosuria, whereas Sirt1 activators are thought to upregulate the highly conserved mechanism, autophagy.
References
-
- Number (in Millions) of Civilian, Noninstitutionalized Adults with Diagnosed Diabetes, United States, 1980–2011, http://www.cdc.gov/diabetes/statistics/prev/national/figadults.htm.
-
- Centers for Disease Control and Prevention. Annual Number (in Thousands) of New Cases of Diagnosed Diabetes Among Adults Aged 18–79 Years, United States, 1980–2011. Centers for Disease Control and Prevention; 2012. http://www.cdc.gov/diabetes/statistics/incidence/fig1.htm.
-
- USRDS: the United States renal data system. American Journal of Kidney Diseases. 2003;42(6, supplement 5):1–230. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
