

Erdheim-Chester Disease: A Case Report
- PMID: 26067743
- PMCID: PMC4479186
- DOI: 10.12659/AJCR.892750
Erdheim-Chester Disease: A Case Report
Abstract
Background: The diagnosis of Erdheim-Chester disease, a rare illness, is difficult and requires increased awareness.
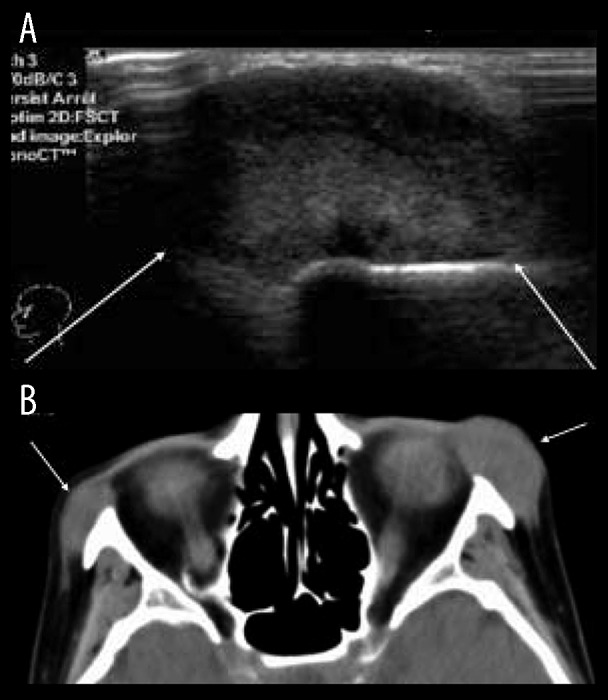
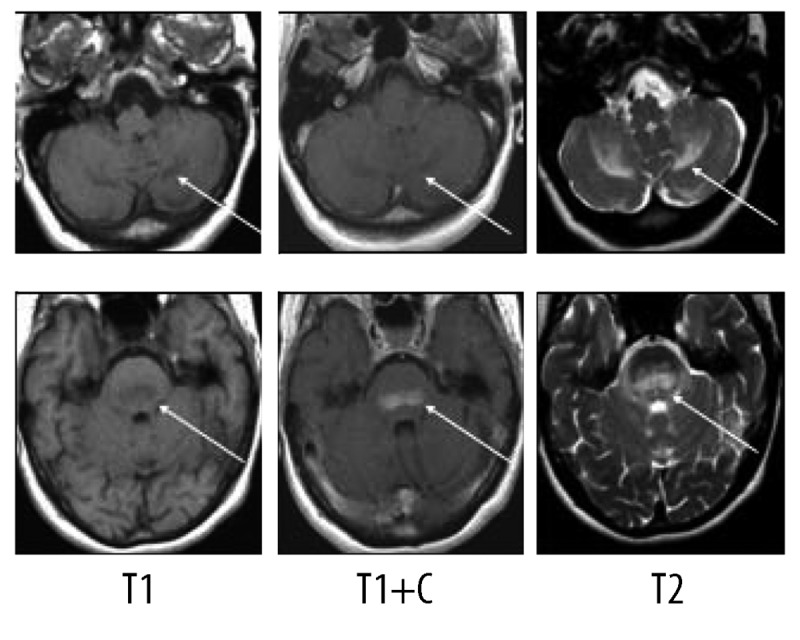
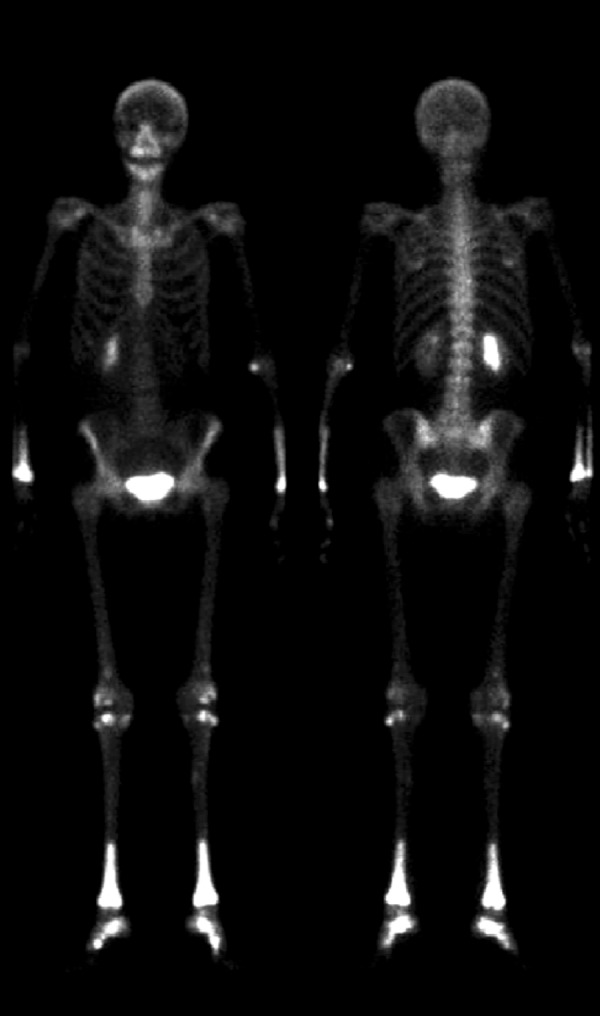
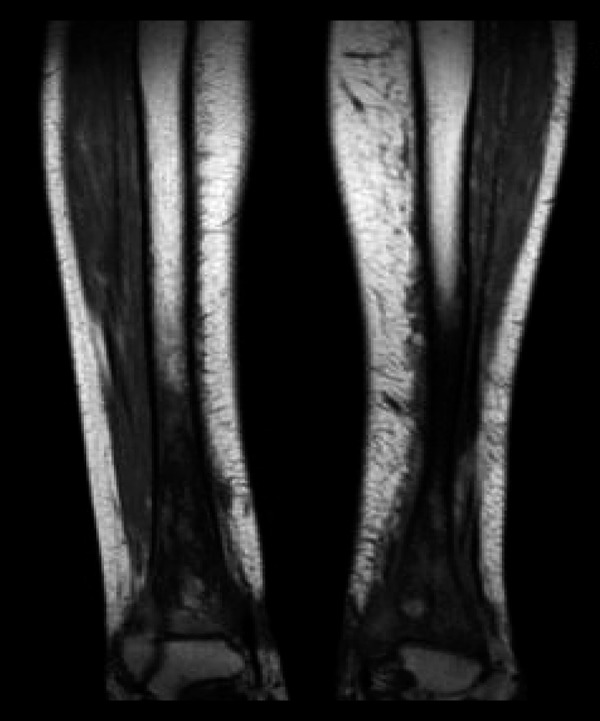
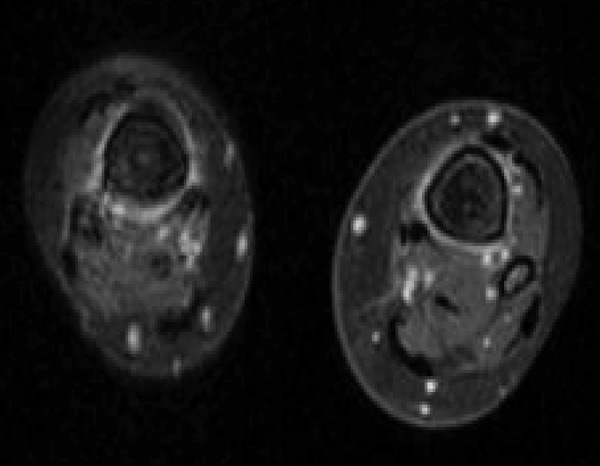
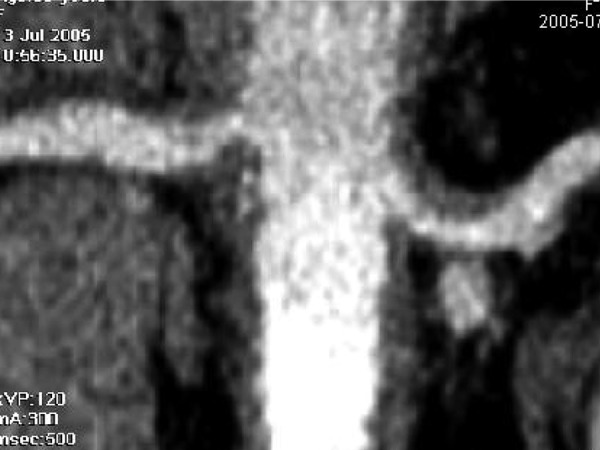
Case report: We report the case of a 56-year-old woman who initially presented with a mesenteric panniculitis and 8 years later developed neurological manifestations and bone lesions that led to a diagnosis of Erdheim-Chester disease.
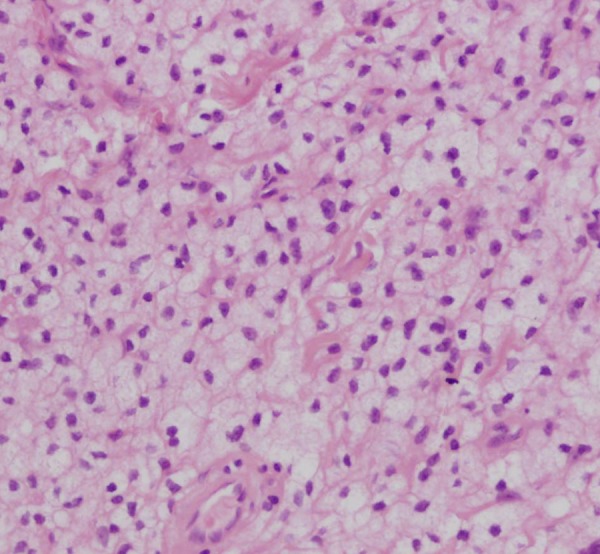
Conclusions: The rather characteristic aspect of the bone lesions as well as the presence of foamy cells in involved tissue biopsies should suggest the diagnosis. No therapy is available at present but recent biological data might suggest new approaches for the understanding and therapy of this condition.
Figures




References
-
- Veyssier-Belot C, Cacoub P, Caparros-Lefebvre D, et al. Erdheim-Chester disease: clinical and radiologic characteristics of 59 cases. Medecine. 1996;75(3):157–69. - PubMed
-
- Gomez C, Diard F, Chateil JF, Moinard M. Imagerie de la maladie d’Erdheim-Chester. J Radiol. 1996;77:1213–21. [in French] - PubMed
-
- Cattin F, Runge M, Nagy N, et al. [Case #5. Erdheim-Chester disease] J Radiol. 2005;86:527–30. [in French] - PubMed
-
- Kenn W, Stäbler A, Zachoval R, et al. Erdheim-Chester disease: a case report and literature overview. Eur Radiol. 1999;9:153–58. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
