

Cytokines in Chronic Rhinosinusitis. Role in Eosinophilia and Aspirin-exacerbated Respiratory Disease
- PMID: 26067893
- PMCID: PMC4595675
- DOI: 10.1164/rccm.201412-2278OC
Cytokines in Chronic Rhinosinusitis. Role in Eosinophilia and Aspirin-exacerbated Respiratory Disease
Abstract
Rationale: The mechanisms that underlie the pathogenesis of chronic rhinosinusitis without nasal polyps (CRSsNP), chronic rhinosinusitis with nasal polyps (CRSwNP), and aspirin-exacerbated respiratory disease (AERD) are not clear.
Objectives: To first evaluate the inflammatory profiles of CRSsNP and CRSwNP tissues and then to investigate whether clinical differences observed between CRSwNP and AERD are in part secondary to differences in inflammatory mediator expression within nasal polyp (NP) tissues.
Methods: Expression levels of numerous inflammatory mediators were determined by quantitative real-time polymerase chain reaction, ELISA, and multiplex immunoassay.
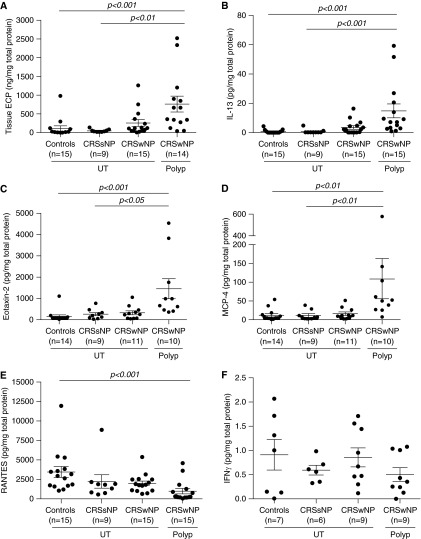
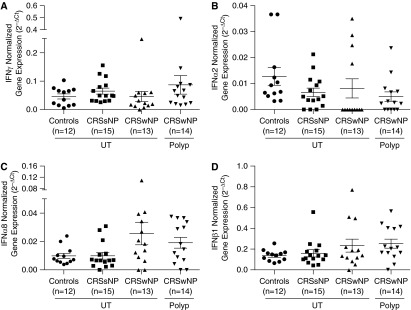
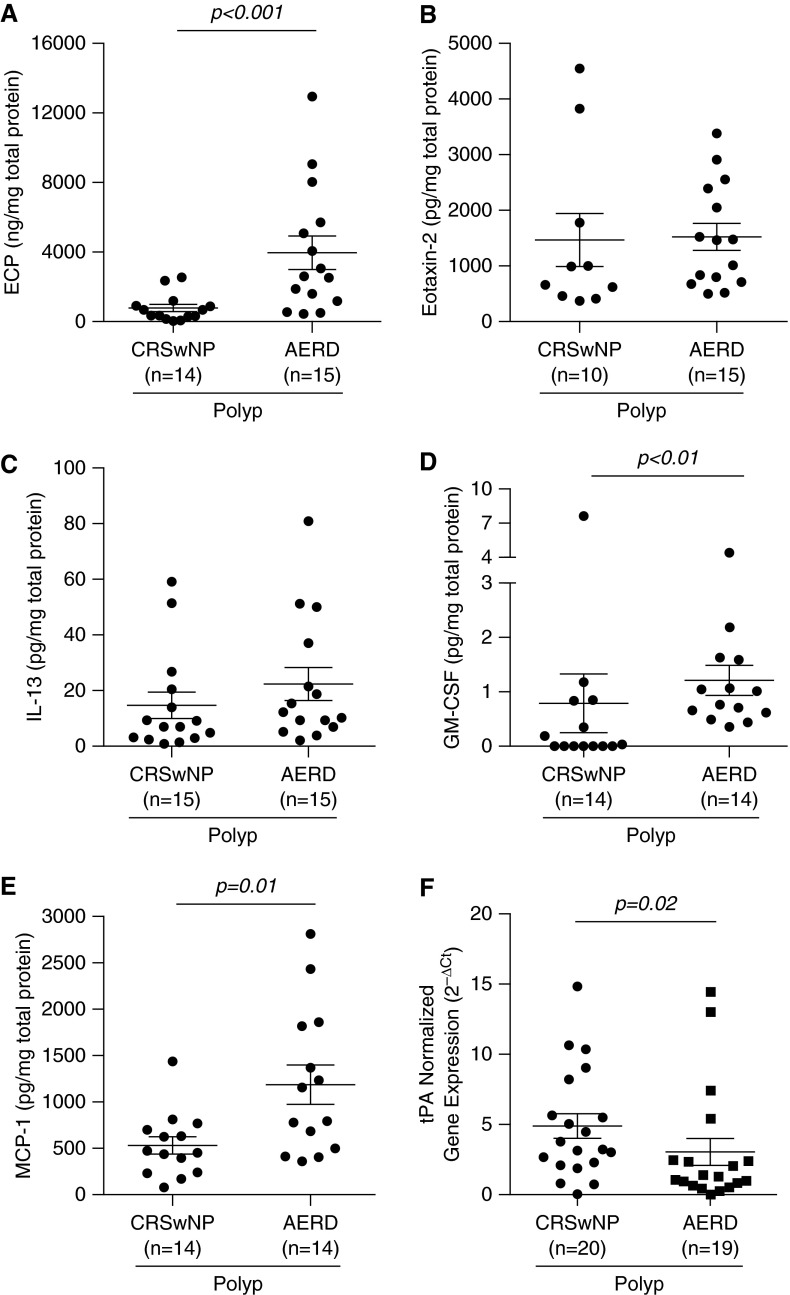
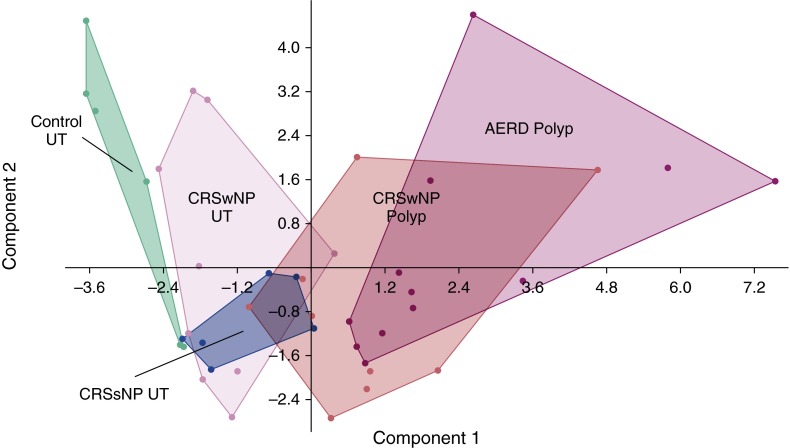
Measurements and main results: CRSwNP NP had increased levels of type 2 mediators, including IL-5 (P < 0.001), IL-13 (P < 0.001), eotaxin-2 (P < 0.001), and monocyte chemoattractant protein (MCP)-4 (P < 0.01), compared with sinonasal tissue from subjects with CRSsNP and control subjects. Expression of IFN-γ messenger RNA or protein was low and not different among the chronic rhinosinusitis subtypes examined. Compared with CRSwNP, AERD NP had elevated protein levels of eosinophil cationic protein (ECP) (P < 0.001), granulocyte-macrophage colony-stimulating factor (GM-CSF) (P < 0.01), and MCP-1 (P = 0.01), as well as decreased gene expression of tissue plasminogen activator (tPA) (P = 0.02). Despite the higher eosinophilia in AERD, there was no associated increase in type 2 mediator protein levels observed.
Conclusions: CRSwNP was characterized by a predominant type 2 inflammatory environment, whereas CRSsNP did not reflect a classic type 1 milieu, as has been suggested previously. AERD can be distinguished from CRSwNP by elevated ECP levels, but this enhanced eosinophilia is not associated with elevations in traditional type 2 inflammatory mediators associated with eosinophil proliferation and recruitment. However, other factors, including GM-CSF, MCP-1, and tPA, may be important contributors to AERD pathogenesis.
Keywords: CRSsNP; CRSwNP; eosinophil.
Figures
Comment in
-
Chronic Rhinosinusitis: More Than Just "Asthma of the Upper Airway".Am J Respir Crit Care Med. 2015 Sep 15;192(6):647-8. doi: 10.1164/rccm.201506-1201ED. Am J Respir Crit Care Med. 2015. PMID: 26371806 Free PMC article. No abstract available.
References
-
- Dykewicz MS, Hamilos DL. Rhinitis and sinusitis. J Allergy Clin Immunol. 2010;125(2) Suppl 2:S103–S115. - PubMed
-
- Bhattacharyya N, Orlandi RR, Grebner J, Martinson M. Cost burden of chronic rhinosinusitis: a claims-based study. Otolaryngol Head Neck Surg. 2011;144:440–445. - PubMed
-
- Fokkens WJ, Lund VJ, Mullol J, Bachert C, Alobid I, Baroody F, Cohen N, Cervin A, Douglas R, Gevaert P, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50:1–12. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
