

Chronic Exposure to Arsenic and Markers of Cardiometabolic Risk: A Cross-Sectional Study in Chihuahua, Mexico
- PMID: 26068977
- PMCID: PMC4710594
- DOI: 10.1289/ehp.1408742
Chronic Exposure to Arsenic and Markers of Cardiometabolic Risk: A Cross-Sectional Study in Chihuahua, Mexico
Abstract
Background: Exposure to arsenic (As) concentrations in drinking water > 150 μg/L has been associated with risk of diabetes and cardiovascular disease, but little is known about the effects of lower exposures.
Objective: This study aimed to examine whether moderate As exposure, or indicators of individual As metabolism at these levels of exposure, are associated with cardiometabolic risk.
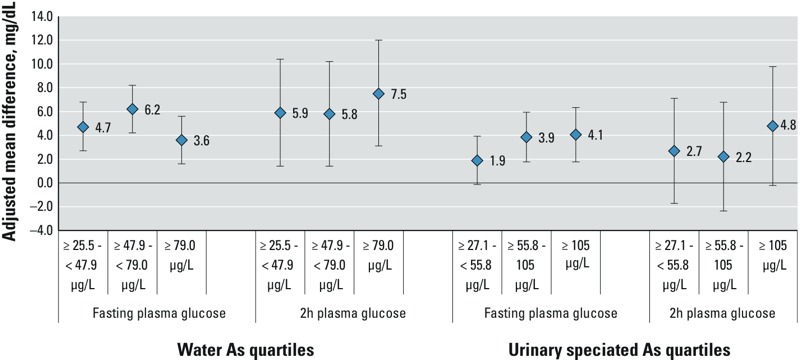
Methods: We analyzed cross-sectional associations between arsenic exposure and multiple markers of cardiometabolic risk using drinking-water As measurements and urinary As species data obtained from 1,160 adults in Chihuahua, Mexico, who were recruited in 2008-2013. Fasting blood glucose and lipid levels, the results of an oral glucose tolerance test, and blood pressure were used to characterize cardiometabolic risk. Multivariable logistic, multinomial, and linear regression were used to assess associations between cardiometabolic outcomes and water As or the sum of inorganic and methylated As species in urine.
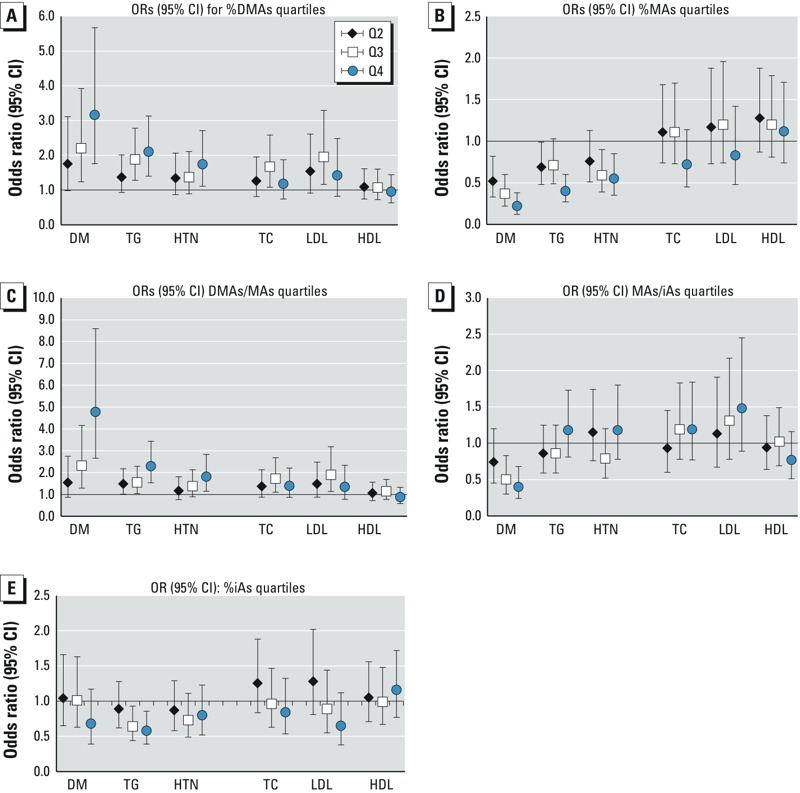
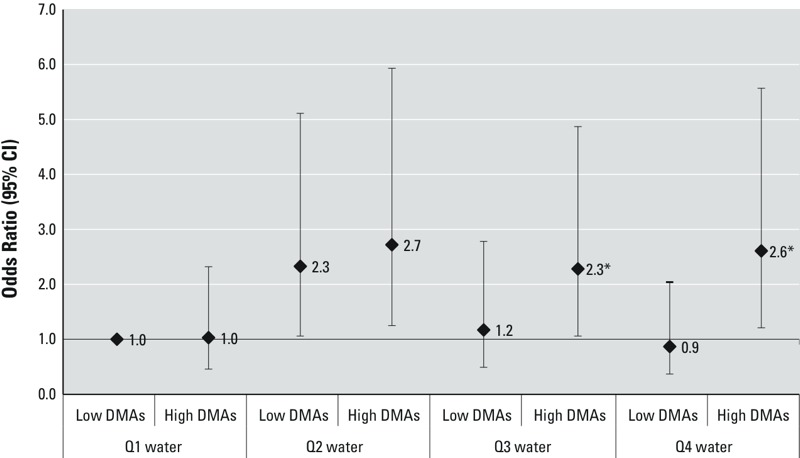
Results: After multivariable adjustment, concentrations in the second quartile of water As (25.5 to < 47.9 μg/L) and concentrations of total speciated urinary As (< 55.8 μg/L) below the median were significantly associated with elevated triglycerides, high total cholesterol, and diabetes. However, moderate water and urinary As levels were also positively associated with HDL cholesterol. Associations between arsenic exposure and both dysglycemia and triglyceridemia were higher among individuals with higher proportions of dimethylarsenic in urine.
Conclusions: Moderate exposure to As may increase cardiometabolic risk, particularly in individuals with high proportions of urinary dimethylarsenic. In this cohort, As exposure was associated with several markers of increased cardiometabolic risk (diabetes, triglyceridemia, and cholesterolemia), but exposure was also associated with higher rather than lower HDL cholesterol.
Citation: Mendez MA, González-Horta C, Sánchez-Ramírez B, Ballinas-Casarrubias L, Hernández Cerón R, Viniegra Morales D, Baeza Terrazas FA, Ishida MC, Gutiérrez-Torres DS, Saunders RJ, Drobná Z, Fry RC, Buse JB, Loomis D, García-Vargas GG, Del Razo LM, Stýblo M. 2016. Chronic exposure to arsenic and markers of cardiometabolic risk: a cross-sectional study in Chihuahua, Mexico. Environ Health Perspect 124:104-111; http://dx.doi.org/10.1289/ehp.1408742.
Conflict of interest statement
The authors declare they have no actual or potential competing financial interests.
Figures
References
-
- Aguilar-Salinas CA, Olaiz G, Valles V, Torres JM, Gómez Pérez FJ, Rull JA, et al. High prevalence of low HDL cholesterol concentrations and mixed hyperlipidemia in a Mexican nationwide survey. J Lipid Res. 2001;42:1298–1307. - PubMed
-
- Ahsan H, Chen Y, Kibriya MG, Slavkovich V, Parvez F, Jasmine F, et al. Arsenic metabolism, genetic susceptibility, and risk of premalignant skin lesions in Bangladesh. Cancer Epidemiol Biomarkers Prev. 2007;16:1270–1278. - PubMed
-
- Barquera S, Campos-Nonato I, Hernández-Barrera L, Flores M, Durazo-Arvizu R, Kanter R, et al. Obesity and central adiposity in Mexican adults: results from the Mexican National Health and Nutrition Survey 2006. Salud Publica Mex. 2009;51(suppl 4):S595–S603. - PubMed
-
- Calatayud M, Gimeno-Alcañiz JV, Vélez D, Devesa V. Trivalent arsenic species induce changes in expression and levels of proinflammatory cytokines in intestinal epithelial cells. Toxicol Lett. 2014;224:40–46. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
