

Robotic Low Ligation of the Inferior Mesenteric Artery for Rectal Cancer Using the Firefly Technique
- PMID: 26069127
- PMCID: PMC4479832
- DOI: 10.3349/ymj.2015.56.4.1028
Robotic Low Ligation of the Inferior Mesenteric Artery for Rectal Cancer Using the Firefly Technique
Abstract
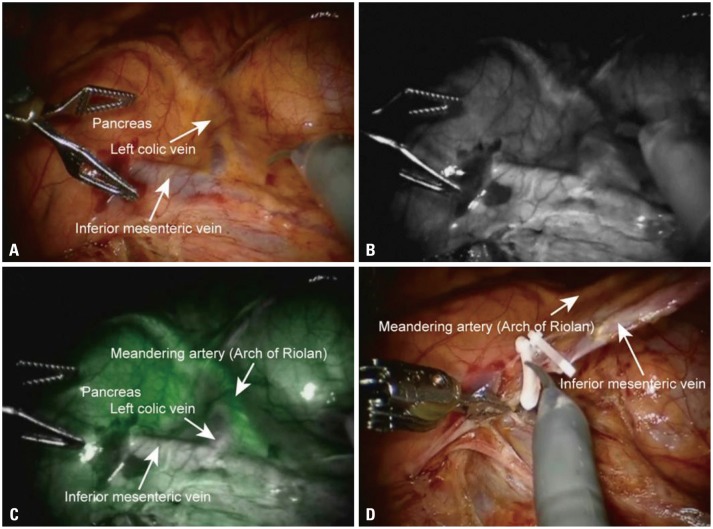
Purpose: By integrating intraoperative near infrared fluorescence imaging into a robotic system, surgeons can identify the vascular anatomy in real-time with the technical advantages of robotics that is useful for meticulous lymphovascular dissection. Herein, we report our initial experience of robotic low ligation of the inferior mesenteric artery (IMA) with real-time identification of the vascular system for rectal cancer using the Firefly technique.
Materials and methods: The study group included 11 patients who underwent a robotic total mesorectal excision with preservation of the left colic artery for rectal cancer using the Firefly technique between July 2013 and December 2013.
Results: The procedures included five low anterior resections and six ultra-low anterior resections with loop ileostomy. The median total operation time was 327 min (226-490). The low ligation time was 10 min (6-20), and the time interval between indocyanine green injection and division of the sigmoid artery was 5 min (2-8). The estimated blood loss was 200 mL (100-500). The median time to soft diet was 4 days (4-5), and the median length of stay was 7 days (5-9). Three patients developed postoperative complications; one patients developed anal stricture, one developed ileus, and one developed non-complicated intraabdominal fluid collection. The median total number of lymph nodes harvested was 17 (9-29).
Conclusion: Robotic low ligation of the IMA with real-time identification of the vascular system for rectal cancer using the Firefly technique is safe and feasible. This technique can allow for precise lymph node dissection along the IMA and facilitate the identification of the left colic branch of the IMA.
Keywords: Robotics; blood supply; colectomy; colonic neoplasm; fluorescence; indocyanine green.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures


References
-
- Kingham TP, Pachter HL. Colonic anastomotic leak: risk factors, diagnosis, and treatment. J Am Coll Surg. 2009;208:269–278. - PubMed
-
- McArdle CS, McMillan DC, Hole DJ. Impact of anastomotic leakage on long-term survival of patients undergoing curative resection for colorectal cancer. Br J Surg. 2005;92:1150–1154. - PubMed
-
- Park YA, Kim JM, Kim SA, Min BS, Kim NK, Sohn SK, et al. Totally robotic surgery for rectal cancer: from splenic flexure to pelvic floor in one setup. Surg Endosc. 2010;24:715–720. - PubMed
-
- Chapuis PH, Dent OF, Fisher R, Newland RC, Pheils MT, Smyth E, et al. A multivariate analysis of clinical and pathological variables in prognosis after resection of large bowel cancer. Br J Surg. 1985;72:698–702. - PubMed
-
- Lindmark G, Gerdin B, Påhlman L, Bergström R, Glimelius B. Prognostic predictors in colorectal cancer. Dis Colon Rectum. 1994;37:1219–1227. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
