

Predicted EC₅₀ and EC₉₅ of Remifentanil for Smooth Removal of a Laryngeal Mask Airway Under Propofol Anesthesia
- PMID: 26069139
- PMCID: PMC4479844
- DOI: 10.3349/ymj.2015.56.4.1128
Predicted EC₅₀ and EC₉₅ of Remifentanil for Smooth Removal of a Laryngeal Mask Airway Under Propofol Anesthesia
Abstract
Purpose: The purpose of this study was to determine the effect-site concentration (Ce) of remifentanil in 50% of patients (EC₅₀) and 95% of patients (EC₉₅) for smooth laryngeal mask airway (LMA) removal in adults under propofol and remifentanil anesthesia.
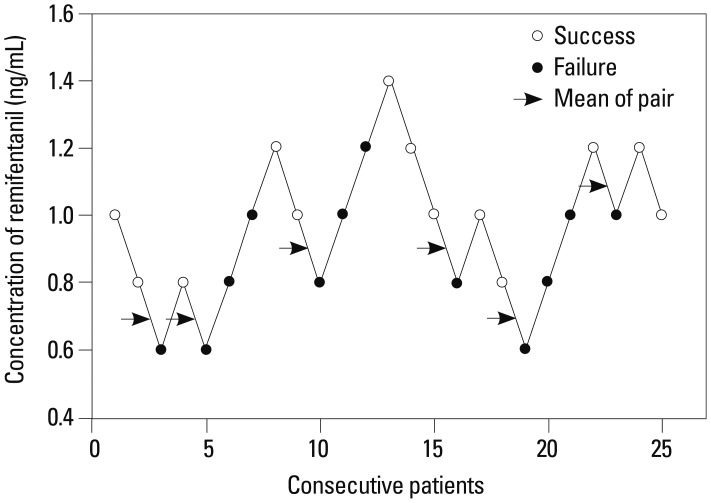
Materials and methods: Twenty-five patients of ASA physical status I-II and ages 18-60 years who were to undergo minor gynecological or orthopedic surgery were assessed in this study. Anesthesia was induced and maintained with propofol and remifentanil target-controlled infusion (TCI). Remifentanil was maintained at a predetermined Ce during the emergence period. The modified Dixon's up-and-down method was used to determine the remifentanil concentration, starting from 1.0 ng/mL (step size of 0.2 ng/mL). Successful removal of the LMA was regarded as absence of coughing/gagging, clenched teeth, gross purposeful movements, breath holding, laryngospasm, or desaturation to SpO₂<90%.
Results: The mean±SD Ce of remifentanil for smooth LMA removal after propofol anesthesia was 0.83±0.16 ng/mL. Using isotonic regression with a bootstrapping approach, the estimated EC₅₀ and EC₉₅ of remifentanil Ce were 0.91 ng/mL [95% confidence interval (CI), 0.77-1.07 ng/mL] and 1.35 ng/mL (95% CI, 1.16-1.38 ng/mL), respectively.
Conclusion: Our results showed that remifentanil TCI at an established Ce is a reliable technique for achieving safe and smooth emergence without coughing, laryngospasm, or other airway reflexes.
Keywords: Laryngeal mask airway; device removal; effect-site concentration; general anesthesia; remifentanil; target-controlled infusion.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Gataure PS, Latto IP, Rust S. Complications associated with removal of the laryngeal mask airway: a comparison of removal in deeply anaesthetised versus awake patients. Can J Anaesth. 1995;42:1113–1116. - PubMed
-
- Pappas AL, Sukhani R, Lurie J, Pawlowski J, Sawicki K, Corsino A. Severity of airway hyperreactivity associated with laryngeal mask airway removal: correlation with volatile anesthetic choice and depth of anesthesia. J Clin Anesth. 2001;13:498–503. - PubMed
-
- Cameron AJ, Sellers WF. Early vs late LMA removal; risks to patients and damage to equipment. Anaesth Intensive Care. 2001;29:80–81. - PubMed
-
- Nunez J, Hughes J, Wareham K, Asai T. Timing of removal of the laryngeal mask airway. Anaesthesia. 1998;53:126–130. - PubMed
-
- Baird MB, Mayor AH, Goodwin AP. Removal of the laryngeal mask airway: factors affecting the incidence of post-operative adverse respiratory events in 300 patients. Eur J Anaesthesiol. 1999;16:251–256. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
