

Normal 25-Hydroxyvitamin D Levels Are Associated with Less Proteinuria and Attenuate Renal Failure Progression in Children with CKD
- PMID: 26069294
- PMCID: PMC4696567
- DOI: 10.1681/ASN.2014090947
Normal 25-Hydroxyvitamin D Levels Are Associated with Less Proteinuria and Attenuate Renal Failure Progression in Children with CKD
Abstract
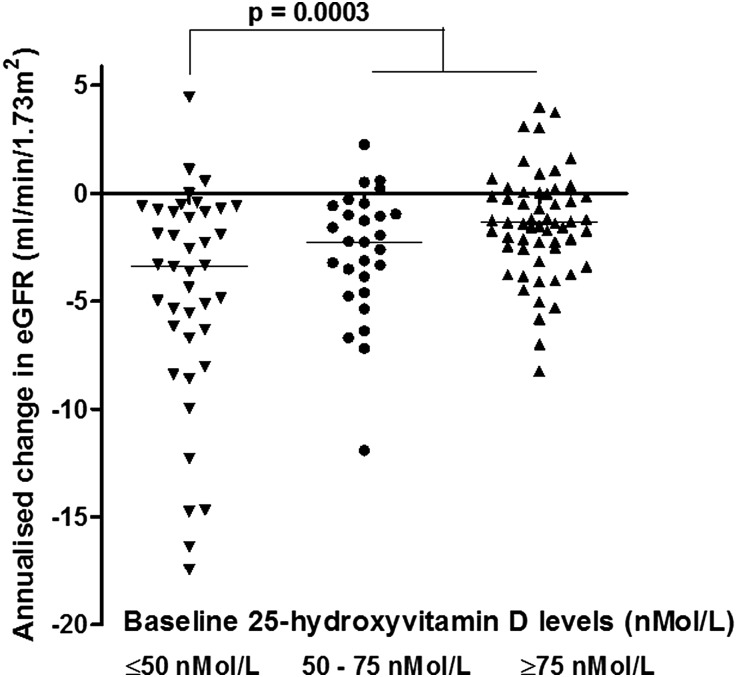
Angiotensin-converting enzyme inhibitors (ACEi) for renin-angiotensin-aldosterone system (RAAS) blockade are routinely used to slow CKD progression. However, vitamin D may also promote renoprotection by suppressing renin transcription through cross-talk between RAAS and vitamin D-fibroblast growth factor-23 (FGF-23)-Klotho pathways. To determine whether vitamin D levels influence proteinuria and CKD progression in children, we performed a post hoc analysis of the Effect of Strict Blood Pressure Control and ACE Inhibition on Progression of CKD in Pediatric Patients (ESCAPE) cohort. In 167 children (median eGFR 51 ml/min per 1.73 m(2)), serum 25-hydroxyvitamin D (25(OH)D), FGF-23, and Klotho levels were measured at baseline and after a median 8 months on ACEi. Children with lower 25(OH)D levels had higher urinary protein/creatinine ratios at baseline (P=0.03) and at follow-up (P=0.006). Levels of 25(OH)D and serum vitamin D-binding protein were not associated, but 25(OH)D ≤50 nmol/L associated with higher diastolic BP (P=0.004). ACEi therapy also associated with increased Klotho levels (P<0.001). The annualized loss of eGFR was inversely associated with baseline 25(OH)D level (P<0.001, r=0.32). Five-year renal survival was 75% in patients with baseline 25(OH)D ≥50 nmol/L and 50% in those with lower 25(OH)D levels (P<0.001). This renoprotective effect remained significant but attenuated with ACEi therapy (P=0.05). Renal survival increased 8.2% per 10 nmol/L increase in 25(OH)D (P=0.03), independent of eGFR; proteinuria, BP, and FGF-23 levels; and underlying renal diagnosis. In children with CKD, 25(OH)D ≥50 nmol/L was associated with greater preservation of renal function. This effect was present but attenuated with concomitant ACEi therapy.
Keywords: ACE inhibitors; children; chronic kidney disease; glomerular filtration rate; proteinuria; vitamin D.
Copyright © 2016 by the American Society of Nephrology.
Figures




References
-
- Remuzzi G, Cattaneo D, Perico N: The aggravating mechanisms of aldosterone on kidney fibrosis. J Am Soc Nephrol 19: 1459–1462, 2008 - PubMed
-
- Ruggenenti P, Schieppati A, Remuzzi G: Progression, remission, regression of chronic renal diseases. Lancet 357: 1601–1608, 2001 - PubMed
-
- Taal MW, Brenner BM: Renoprotective benefits of RAS inhibition: from ACEI to angiotensin II antagonists. Kidney Int 57: 1803–1817, 2000 - PubMed
-
- Wühl E, Trivelli A, Picca S, Litwin M, Peco-Antic A, Zurowska A, Testa S, Jankauskiene A, Emre S, Caldas-Afonso A, Anarat A, Niaudet P, Mir S, Bakkaloglu A, Enke B, Montini G, Wingen AM, Sallay P, Jeck N, Berg U, Caliskan S, Wygoda S, Hohbach-Hohenfellner K, Dusek J, Urasinski T, Arbeiter K, Neuhaus T, Gellermann J, Drozdz D, Fischbach M, Möller K, Wigger M, Peruzzi L, Mehls O, Schaefer F, ESCAPE Trial Group : Strict blood-pressure control and progression of renal failure in children. N Engl J Med 361: 1639–1650, 2009 - PubMed
-
- Ruggenenti P, Perna A, Remuzzi G, GISEN Group Investigators : Retarding progression of chronic renal disease: the neglected issue of residual proteinuria. Kidney Int 63: 2254–2261, 2003 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
