

¹⁸F-DCFBC PET/CT for PSMA-Based Detection and Characterization of Primary Prostate Cancer
- PMID: 26069305
- PMCID: PMC4659400
- DOI: 10.2967/jnumed.115.154336
¹⁸F-DCFBC PET/CT for PSMA-Based Detection and Characterization of Primary Prostate Cancer
Abstract
We previously demonstrated the ability to detect metastatic prostate cancer using N-[N-[(S)-1,3-dicarboxypropyl]carbamoyl]-4-(18)F-fluorobenzyl-L-cysteine ((18)F-DCFBC), a low-molecular-weight radiotracer that targets the prostate-specific membrane antigen (PSMA). PSMA has been shown to be associated with higher Gleason grade and more aggressive disease. An imaging biomarker able to detect clinically significant high-grade primary prostate cancer reliably would address an unmet clinical need by allowing for risk-adapted patient management.
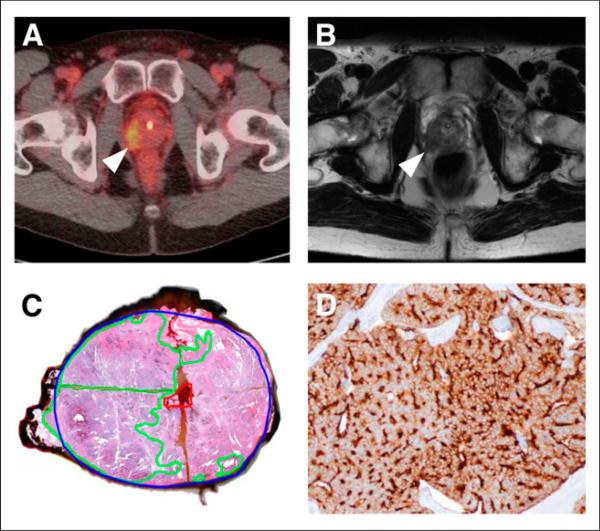
Methods: We enrolled 13 patients with primary prostate cancer who were imaged with (18)F-DCFBC PET before scheduled prostatectomy, with 12 of these patients also undergoing pelvic prostate MR imaging. Prostate (18)F-DCFBC PET was correlated with MR imaging and histologic and immunohistochemical analysis on a prostate-segment (12 regions) and dominant-lesion basis. There were no incidental extraprostatic findings on PET suggestive of metastatic disease.
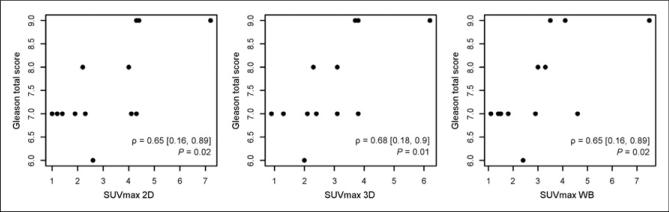
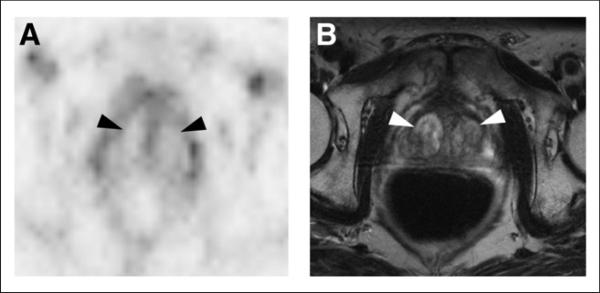
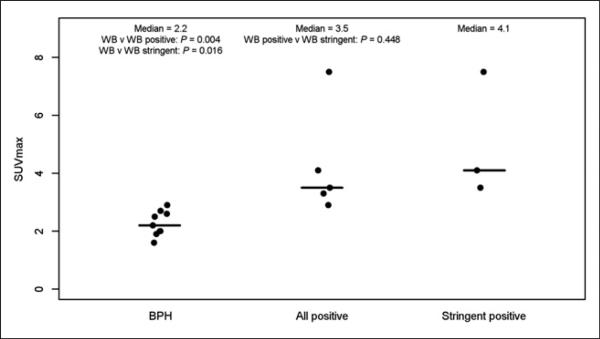
Results: MR imaging was more sensitive than (18)F-DCFBC PET for detection of primary prostate cancer on a per-segment (sensitivities of up to 0.17 and 0.39 for PET and MR imaging, respectively) and per-dominant-lesion analysis (sensitivities of 0.46 and 0.92 for PET and MR imaging, respectively). However, (18)F-DCFBC PET was more specific than MR imaging by per-segment analysis (specificities of 0.96 and 0.89 for PET and MR imaging for corresponding sensitivity, respectively) and specific for detection of high-grade lesions (Gleason 8 and 9) greater than 1.0 mL in size (4/4 of these patients positive by PET). (18)F-DCFBC uptake in tumors was positively correlated with Gleason score (ρ = 0.64; PSMA expression, ρ = 0.47; and prostate-specific antigen, ρ = 0.52). There was significantly lower (18)F-DCFBC uptake in benign prostatic hypertrophy than primary tumors (median maximum standardized uptake value, 2.2 vs. 3.5; P = 0.004).
Conclusion: Although the sensitivity of (18)F-DCFBC for primary prostate cancer was less than MR imaging, (18)F-DCFBC PET was able to detect the more clinically significant high-grade and larger-volume tumors (Gleason score 8 and 9) with higher specificity than MR imaging. In particular, there was relatively low (18)F-DCFBC PET uptake in benign prostatic hypertrophy lesions, compared with cancer in the prostate, which may allow for more specific detection of primary prostate cancer by (18)F-DCFBC PET. This study demonstrates the utility of PSMA-based PET, which may be used in conjunction with MR imaging to identify clinically significant prostate cancer.
Trial registration: ClinicalTrials.gov NCT01496157.
Keywords: MRI; PET/CT; primary prostate cancer; prostate specific membrane antigen (PSMA); prostatectomy.
© 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
Figures
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64:9–29. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous