

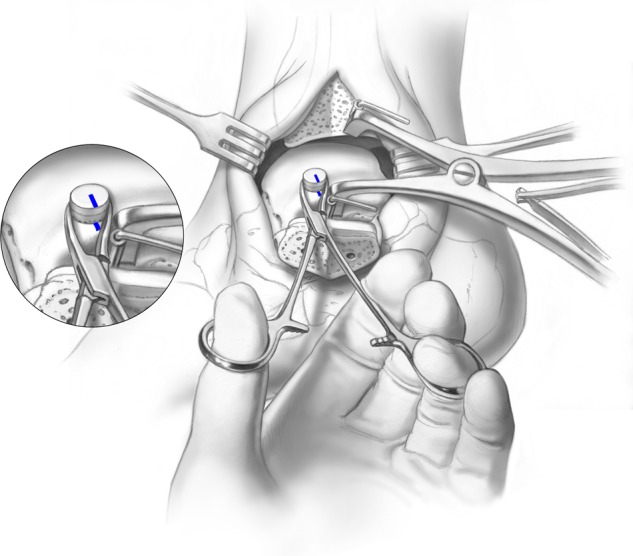
The Treatment of Osteochondral Lesions of the Talus with Autologous Osteochondral Transplantation and Bone Marrow Aspirate Concentrate: Surgical Technique
- PMID: 26069591
- PMCID: PMC4297142
- DOI: 10.1177/1947603511400726
The Treatment of Osteochondral Lesions of the Talus with Autologous Osteochondral Transplantation and Bone Marrow Aspirate Concentrate: Surgical Technique
Abstract
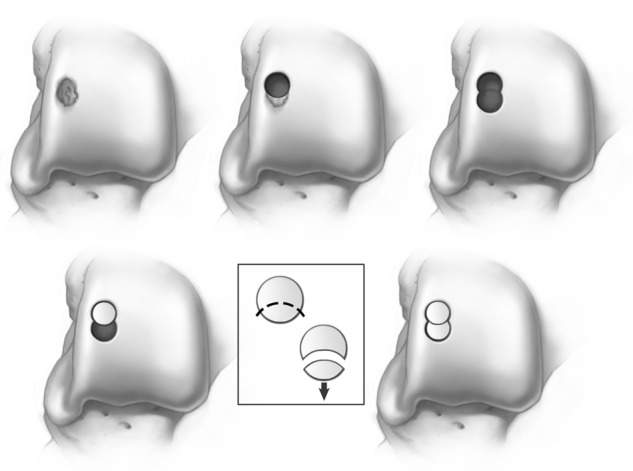
Objective: To present the functional results after autologous osteochondral transplantation with bone marrow aspirate concentrate in 72 patients, while placing an emphasis on the surgical technique.
Methods: Between 2005 and 2009, 72 patients underwent autologous osteochondral transplantation under the care of the senior author. The mean patient age at the time of surgery was 34.19 years (range, 16-85 years). All patients were followed for a minimum of 1 year after surgery. The mean follow-up time was 28.02 months (range, 12-64 months). Patient-reported outcome measures were taken preoperatively and at final follow-up using the Foot and Ankle Outcome Score (FAOS) and Short Form-12 (SF-12) general health questionnaire. Identical questionnaires were used in all instances.
Results: The mean FAOS scores improved from 52.67 points preoperatively to 86.19 points postoperatively (range, 71-100 points). The mean SF-12 scores also improved from 59.40 points preoperatively to 88.63 points postoperatively (range, 52-98 points). Three patients reported donor site knee pain after surgery, and one patient required the decompression of a cyst that developed beneath the graft site approximately 2 years after the index procedure.
Conclusion: Autologous osteochondral transplantation is a reproducible and primary treatment strategy for large osteochondral lesions of the talus.
Keywords: ankle < joint involved; articular cartilage < tissue; cartilage repair < repair; cartilage transplantation < grafts; sports injury < diagnosis.
Conflict of interest statement
Figures

References
-
- Saxena A, Eakin C. Articular talar injuries in athletes: results of microfracture and autogenous bone graft. Am J Sports Med. 2007;35(10):1680-7. - PubMed
-
- Karlsson J, Sancone M. Management of acute ligament injuries of the ankle. Foot Ankle Clin. 2006;11(3):521-30. - PubMed
-
- Kannus P, Renstrom P. Treatment for acute tears of the lateral ligaments of the ankle: operation, cast, or early controlled mobilization. J Bone Joint Surg Am. 1991;73(2):305-12. - PubMed
-
- Lynch SA, Renström PA. Treatment of acute lateral ankle ligament rupture in the athlete conservative versus surgical treatment. Sports Med. 1999;27(1):61-71. - PubMed
-
- Chuckpaiwong B, Berkson EM, Theodore GH. Microfracture for osteochondral lesions of the ankle: outcome analysis and outcome predictors of 105 cases. Arthroscopy. 2008;24: 106-12. - PubMed
LinkOut - more resources
Full Text Sources
Medical
