

Magnesium in chronic kidney disease Stages 3 and 4 and in dialysis patients
- PMID: 26069820
- PMCID: PMC4455820
- DOI: 10.1093/ndtplus/sfr166
Magnesium in chronic kidney disease Stages 3 and 4 and in dialysis patients
Abstract
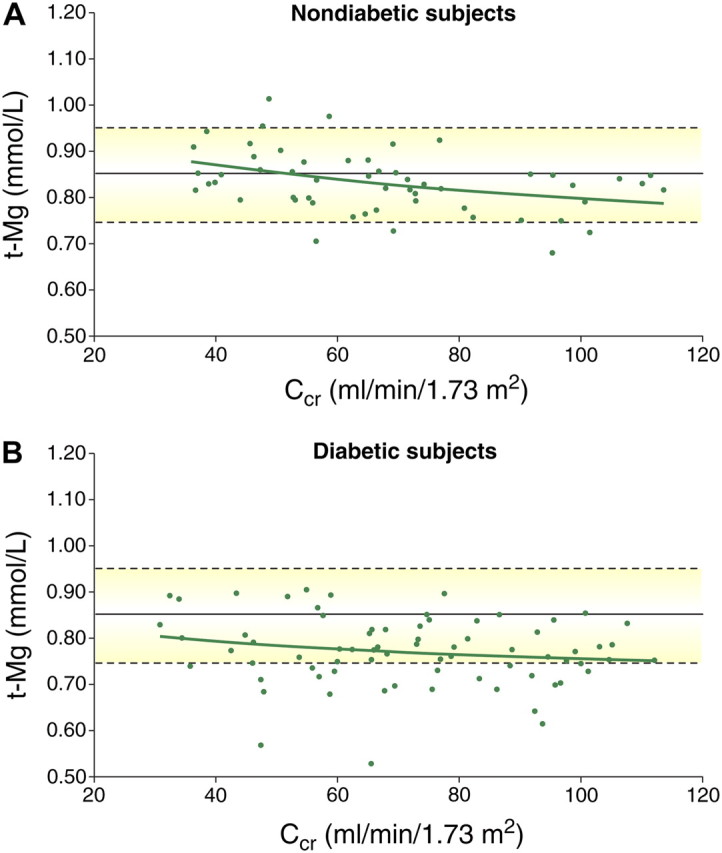
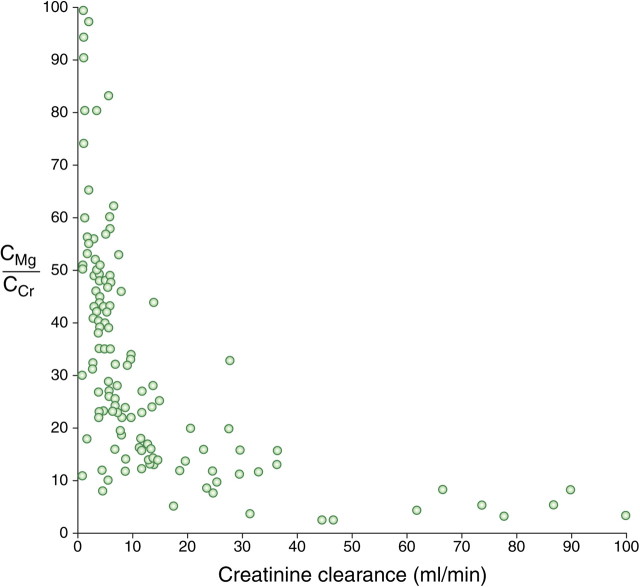
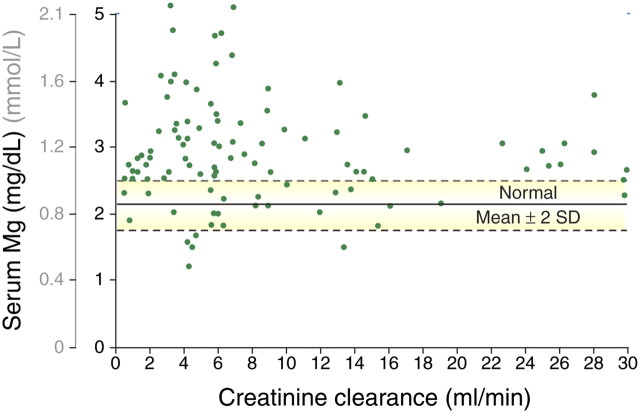
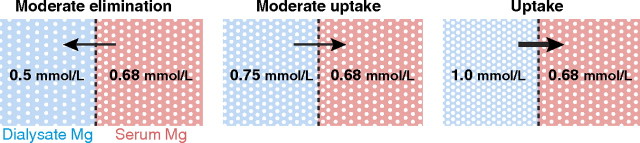
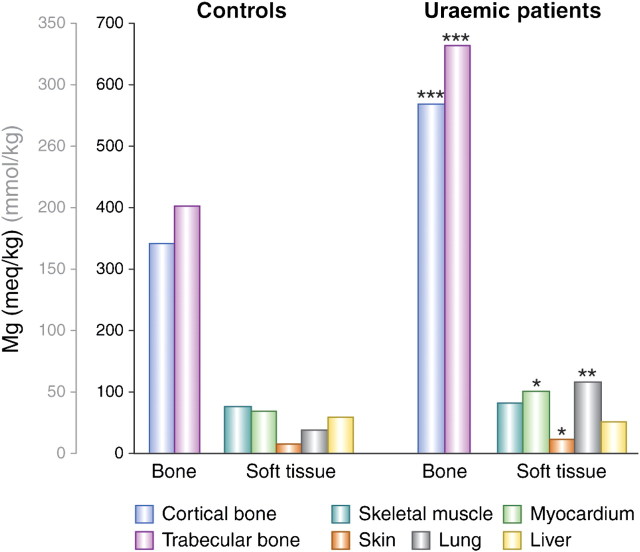
The kidney has a vital role in magnesium homeostasis and, although the renal handling of magnesium is highly adaptable, this ability deteriorates when renal function declines significantly. In moderate chronic kidney disease (CKD), increases in the fractional excretion of magnesium largely compensate for the loss of glomerular filtration rate to maintain normal serum magnesium levels. However, in more advanced CKD (as creatinine clearance falls <30 mL/min), this compensatory mechanism becomes inadequate such that overt hypermagnesaemia develops frequently in patients with creatinine clearances <10 mL/min. Dietary calcium and magnesium may affect the intestinal uptake of each other, though results are conflicting, and likewise the role of vitamin D on intestinal magnesium absorption is somewhat uncertain. In patients undergoing dialysis, the effect of various magnesium and calcium dialysate concentrations has been investigated in haemodialysis (HD) and peritoneal dialysis (PD). Results generally show that dialysate magnesium, at 0.75 mmol/L, is likely to cause mild hypermagnesaemia, results for a magnesium dialysate concentration of 0.5 mmol/L were less consistent, whereas serum magnesium levels were mostly normal to hypomagnesaemic when 0.2 and 0.25 mmol/L were used. While dialysate magnesium concentration is a major determinant of HD or PD patients' magnesium balance, other factors such as nutrition and medications (e.g. laxatives or antacids) also play an important role. Also examined in this review is the role of magnesium on parathyroid hormone (PTH) levels in dialysis patients. Although various studies have shown that patients with higher serum magnesium tend to have lower PTH levels, many of these suffer from methodological limitations. Finally, we examine the complex and often conflicting results concerning the interplay between magnesium and bone in uraemic patients. Although the exact role of magnesium in bone metabolism is unclear, it may have both positive and negative effects, and it is uncertain what the optimal magnesium levels are in uraemic patients.
Keywords: CKD; bone; dialysate magnesium; diuretics; haemodialysis; magnesium; magnesium supplements; peritoneal dialysis.
Figures
Similar articles
-
Why are serum magnesium levels lower in Saudi dialysis patients?J Taibah Univ Med Sci. 2016 Oct 15;12(1):41-46. doi: 10.1016/j.jtumed.2016.08.008. eCollection 2017 Feb. J Taibah Univ Med Sci. 2016. PMID: 31435211 Free PMC article.
-
To evaluate the relationship between serum magnesium and parathyroid hormone levels in peritoneal dialysis and hemodialysis patients.Int Urol Nephrol. 2023 May;55(5):1321-1327. doi: 10.1007/s11255-022-03445-5. Epub 2022 Dec 16. Int Urol Nephrol. 2023. PMID: 36526918
-
Magnesium metabolism in chronic renal failure.Magnes Res. 1990 Jun;3(2):121-7. Magnes Res. 1990. PMID: 2133626 Review.
-
Inverse correlation between serum magnesium and parathyroid hormone in peritoneal dialysis patients: a contributing factor to adynamic bone disease?Int Urol Nephrol. 2006;38(2):317-22. doi: 10.1007/s11255-006-0082-6. Int Urol Nephrol. 2006. PMID: 16868704 Clinical Trial.
-
1alpha(OH)D3 One-alpha-hydroxy-cholecalciferol--an active vitamin D analog. Clinical studies on prophylaxis and treatment of secondary hyperparathyroidism in uremic patients on chronic dialysis.Dan Med Bull. 2008 Nov;55(4):186-210. Dan Med Bull. 2008. PMID: 19232159 Review.
Cited by
-
Serum magnesium concentrations in patients receiving sodium picosulfate and magnesium citrate bowel preparation: an assessment of renal function and electrocardiographic conduction.Clin Exp Gastroenterol. 2015 Jul 28;8:215-24. doi: 10.2147/CEG.S79216. eCollection 2015. Clin Exp Gastroenterol. 2015. PMID: 26251626 Free PMC article.
-
The Role of Bone Biopsy in the Management of CKD-MBD.Calcif Tissue Int. 2021 Apr;108(4):528-538. doi: 10.1007/s00223-021-00838-z. Epub 2021 Mar 26. Calcif Tissue Int. 2021. PMID: 33772341 Review.
-
Morphological and clinical findings in Sri Lankan patients with chronic kidney disease of unknown cause (CKDu): Similarities and differences with Mesoamerican Nephropathy.PLoS One. 2018 Mar 7;13(3):e0193056. doi: 10.1371/journal.pone.0193056. eCollection 2018. PLoS One. 2018. PMID: 29513702 Free PMC article.
-
Paradoxical Inadequate Parathyroid Hormone Secretion Secondary to Severe Hypomagnesemia: A Review of the Literature.Kidney Med. 2025 Jun 14;7(8):101046. doi: 10.1016/j.xkme.2025.101046. eCollection 2025 Aug. Kidney Med. 2025. PMID: 40740723 Free PMC article. Review.
-
Magnesium Improves Cardiac Function in Experimental Uremia by Altering Cardiac Elastin Protein Content.Nutrients. 2023 Mar 7;15(6):1303. doi: 10.3390/nu15061303. Nutrients. 2023. PMID: 36986034 Free PMC article.
References
-
- Saha HH, Harmoinen AP, Pasternack AI. Measurement of serum ionized magnesium in CAPD patients. Perit Dial Int. 1997;17:347–352. - PubMed
-
- Massry SG, Seelig MS. Hypomagnesemia and hypermagnesemia. Clin Nephrol. 1977;7:147–153. - PubMed
-
- Mordes JP, Wacker WE. Excess magnesium. Pharmacol Rev. 1977;29:273–300. - PubMed
-
- Lembcke B, Fuchs C. Magnesium load induced by ingestion of magnesium-containing antacids. Contrib Nephrol. 1984;38:185–194. - PubMed
-
- Castelbaum AR, Donofrio PD, Walker FO, Troost BT. Laxative abuse causing hypermagnesemia, quadriparesis, and neuromuscular junction defect. Neurology. 1989;39:746–747. - PubMed
LinkOut - more resources
Full Text Sources
