

Use of magnesium as a drug in chronic kidney disease
- PMID: 26069822
- PMCID: PMC4455824
- DOI: 10.1093/ndtplus/sfr168
Use of magnesium as a drug in chronic kidney disease
Abstract
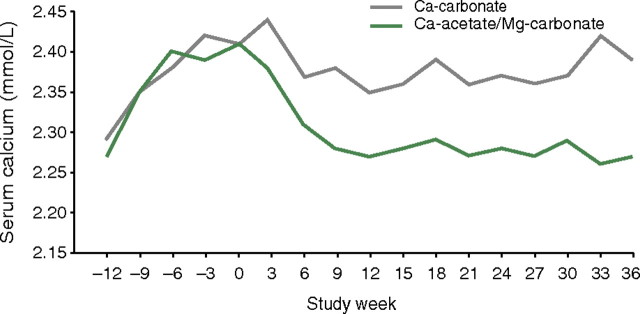
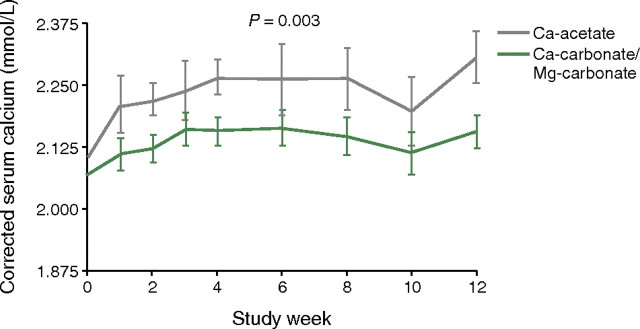
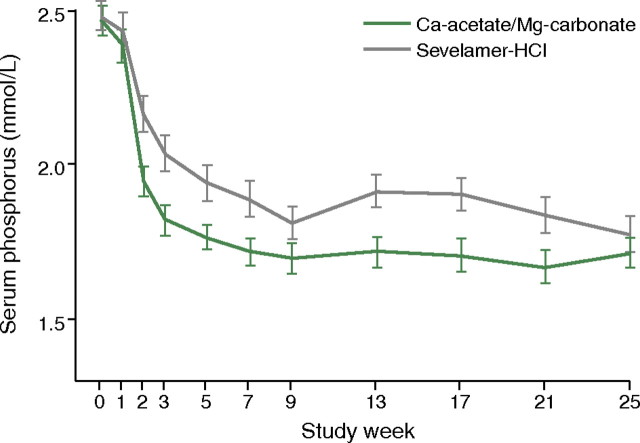
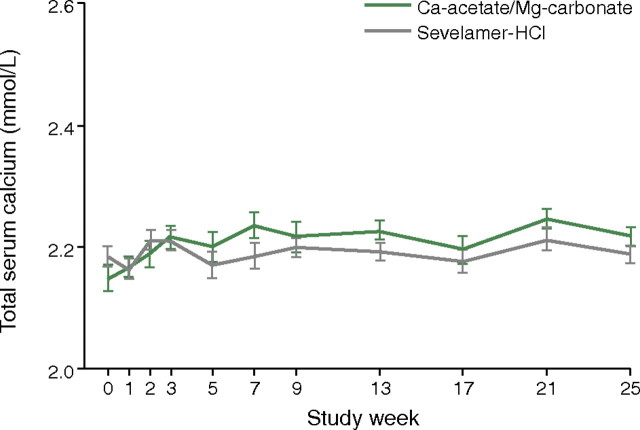
From chronic kidney disease (CKD) Stage 4 onwards, phosphate binders are needed in many patients to prevent the development of hyperphosphataemia, which can result in disturbed bone and mineral metabolism, cardiovascular disease and secondary hyperparathyroidism. In this review, we re-examine the use of magnesium-containing phosphate binders for patients with CKD, particularly as their use circumvents problems such as calcium loading, aluminum toxicity and the high costs associated with other agents of this class. The use of magnesium hydroxide in the 1980s has been superseded by magnesium carbonate, as the hydroxide salt was associated with poor gastrointestinal tolerability, whereas studies with magnesium carbonate show much better gastrointestinal profiles. The use of combined magnesium- and calcium-based phosphate binder regimens allows a reduction in the calcium load, and magnesium and calcium regimen comparisons show that magnesium may be as effective a phosphate binder as calcium. A large well-designed trial has recently shown that a drug combining calcium acetate and magnesium carbonate was non-inferior in terms of lowering serum phosphate to sevelamer-HCl and had an equally good tolerability profile. Because of the high cost of sevelamer and lanthanum carbonate, the use of magnesium carbonate could be advantageous and drug acquisition cost savings would compensate for the cost of introducing routine magnesium monitoring, if this is thought to be necessary and not performed anyway. Moreover, given the potential cost savings, it may be time to re-investigate magnesium-containing phosphate binders for CKD patients with further well-designed clinical research using vascular end points.
Keywords: chronic kidney disease; cost-effectiveness; magnesium; phosphate binder.
Figures
Similar articles
-
Influence of pH and phosphate concentration on the phosphate binding capacity of five contemporary binders. An in vitro study.Nephrology (Carlton). 2019 Feb;24(2):221-226. doi: 10.1111/nep.13245. Epub 2018 Apr 6. Nephrology (Carlton). 2019. PMID: 29479762 Free PMC article.
-
[Changes in mineral metabolism in stage 3, 4, and 5 chronic kidney disease (not on dialysis)].Nefrologia. 2008;28 Suppl 3:67-78. Nefrologia. 2008. PMID: 19018742 Spanish.
-
Clinical Evaluation of the Safety, Efficacy and Tolerability of Lanthanum Carbonate in the Management of Hyperphosphatemia in Patients with End-Stage Renal Disease.Ther Clin Risk Manag. 2020 Sep 15;16:871-880. doi: 10.2147/TCRM.S196805. eCollection 2020. Ther Clin Risk Manag. 2020. PMID: 32982259 Free PMC article. Review.
-
A comparative review of the efficacy and safety of established phosphate binders: calcium, sevelamer, and lanthanum carbonate.Curr Med Res Opin. 2007 Dec;23(12):3167-75. doi: 10.1185/030079907X242719. Curr Med Res Opin. 2007. PMID: 17991307 Review.
-
Cost-Effectiveness of First-Line Sevelamer and Lanthanum versus Calcium-Based Binders for Hyperphosphatemia of Chronic Kidney Disease.Value Health. 2018 Mar;21(3):318-325. doi: 10.1016/j.jval.2017.08.3020. Epub 2017 Oct 18. Value Health. 2018. PMID: 29566839
Cited by
-
Phosphate binders in chronic kidney disease: a systematic review of recent data.J Nephrol. 2016 Jun;29(3):329-340. doi: 10.1007/s40620-016-0266-9. Epub 2016 Jan 22. J Nephrol. 2016. PMID: 26800972
-
Near death by milk of magnesia.BMJ Case Rep. 2017 Mar 21;2017:bcr2016218260. doi: 10.1136/bcr-2016-218260. BMJ Case Rep. 2017. PMID: 28325719 Free PMC article.
-
Magnesium in chronic kidney disease Stages 3 and 4 and in dialysis patients.Clin Kidney J. 2012 Feb;5(Suppl 1):i39-i51. doi: 10.1093/ndtplus/sfr166. Clin Kidney J. 2012. PMID: 26069820 Free PMC article.
-
Magnesium prevents phosphate-induced calcification in human aortic vascular smooth muscle cells.Nephrol Dial Transplant. 2013 Apr;28(4):869-78. doi: 10.1093/ndt/gfs520. Epub 2012 Dec 9. Nephrol Dial Transplant. 2013. PMID: 23229924 Free PMC article.
-
Phosphate recovery from water using cellulose enhanced magnesium carbonate pellets: Kinetics, isotherms, and desorption.Chem Eng J. 2018 Nov 15;352:612-624. doi: 10.1016/j.cej.2018.06.183. Chem Eng J. 2018. PMID: 32831624 Free PMC article.
References
-
- Rees L, Shroff RC. Phosphate binders in CKD: chalking out the differences. Pediatr Nephrol. 2010;25:385–394. - PubMed
-
- Moe SM, Chen NX. Pathophysiology of vascular calcification in chronic kidney disease. Circ Res. 2004;95:560–567. - PubMed
-
- Moe SM. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Kidney Int Suppl. 2009;76:S1–S130. - PubMed
-
- National Kidney Foundation Inc. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis. 2003;42:S1–S201. - PubMed
-
- Hutchison AJ. Oral phosphate binders. Kidney Int. 2009;75:906–914. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
