

Identifying an Optimal Cutpoint for the Diagnosis of Hypertriglyceridemia in the Nonfasting State
- PMID: 26071491
- PMCID: PMC4554926
- DOI: 10.1373/clinchem.2015.241752
Identifying an Optimal Cutpoint for the Diagnosis of Hypertriglyceridemia in the Nonfasting State
Abstract
Background: Nonfasting triglycerides are similar or superior to fasting triglycerides at predicting cardiovascular events. However, diagnostic cutpoints are based on fasting triglycerides. We examined the optimal cutpoint for increased nonfasting triglycerides.
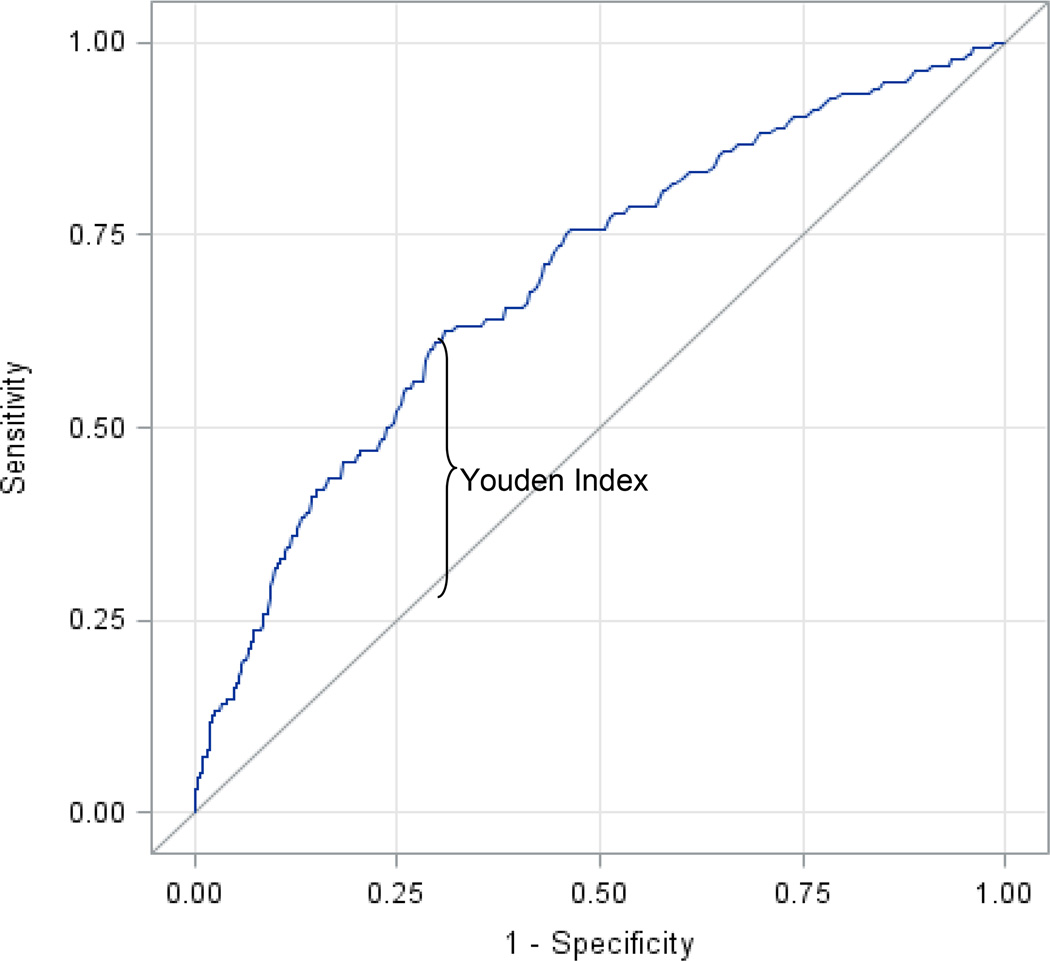
Methods: We obtained baseline nonfasting (<8 h since last meal) samples from 6391 participants in the Women's Health Study who were followed prospectively for ≤17 years. The optimal diagnostic threshold for nonfasting triglycerides, determined by logistic regression models by use of c-statistics and the Youden index (sum of sensitivity and specificity minus 1), was used to calculate hazard ratios (HRs) for incident cardiovascular events. Performance was compared to thresholds recommended by the American Heart Association (AHA) and European guidelines.
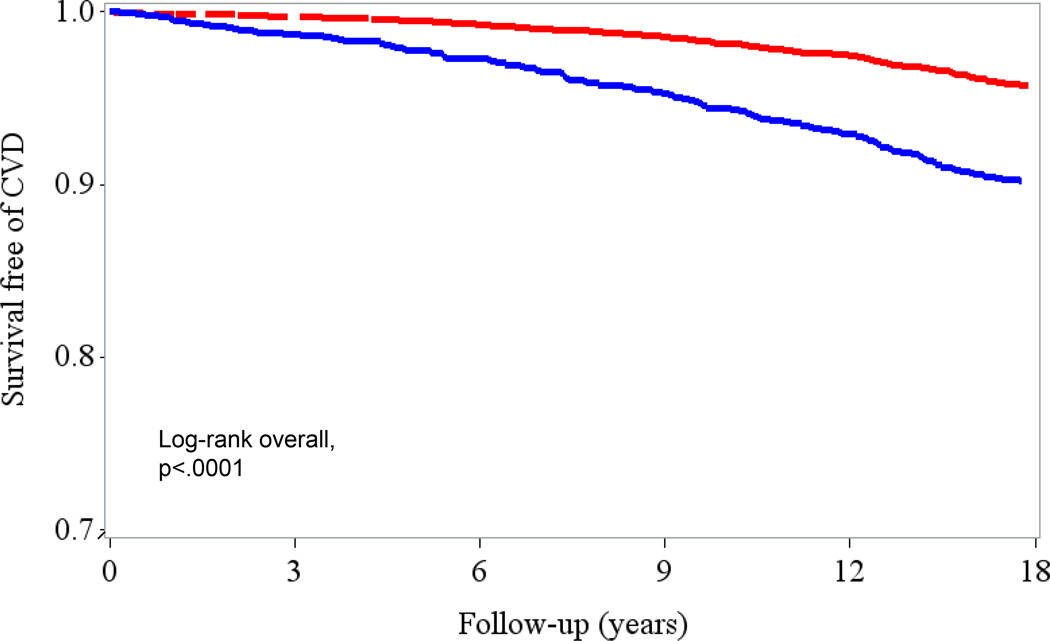
Results: The optimal threshold was 175 mg/dL (1.98 mmol/L), with a c-statistic of 0.656, statistically better than the AHA cutpoint of 200 mg/dL (c-statistic 0.628). For nonfasting triglycerides above and below 175 mg/dL, after adjusting for age, hypertension, smoking, hormone use, and menopausal status, the HR for cardiovascular events was 1.88 (95% CI 1.52-2.33, P < 0.001), and for triglycerides measured at 0-4 and 4-8 h since the last meal, 2.05 (1.54- 2.74) and 1.68 (1.21-2.32), respectively. We validated performance of this optimal cutpoint by use of 10-fold cross-validation and bootstrapping of multivariable models that included standard risk factors plus total and HDL cholesterol, diabetes, body mass index, and C-reactive protein.
Conclusions: In this study of middle-aged and older apparently healthy women, we identified a diagnostic threshold for nonfasting hypertriglyceridemia of 175 mg/dL (1.98 mmol/L), with the potential to more accurately identify cases than the currently recommended AHA cutpoint.
© 2015 American Association for Clinical Chemistry.
Figures
Comment in
-
Nonfasting Lipid Profiles: The Way of the Future.Clin Chem. 2015 Sep;61(9):1123-5. doi: 10.1373/clinchem.2015.243139. Epub 2015 Jul 23. Clin Chem. 2015. PMID: 26206883 No abstract available.
References
-
- Nordestgaard BG, Varbo A. Triglycerides and cardiovascular disease. Lancet. 2014;384:626–635. - PubMed
-
- Shai I, Rimm EB, Hankinson SE, Cannuscio C, Curhan G, Manson JE, Rifai N, Stampfer MJ, Ma J. Lipoprotein (a) and coronary heart disease among women: Beyond a cholesterol carrier? Eur Heart J. 2005;26:1633–1639. - PubMed
-
- Ridker PM, Rifai N, Cook NR, Bradwin G, Buring JE. Non-HDL cholesterol, apolipoproteins A-I and B100, standard lipid measures, lipid ratios, and CRP as risk factors for cardiovascular disease in women. JAMA. 2005;294:326–333. - PubMed
-
- Alipour A, van Oostrom AJHHM, Izraeljan A, Verseyden C, Collins JM, Frayn KN, Plokker TWM, Elte JWF, Castro Cabezas M. Leukocyte activation by triglyceride-rich lipoproteins. Arterioscler Thromb Vasc Biol. 2008;28:792–797. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
