

Thyroid function in critically ill patients
- PMID: 26071885
- PMCID: PMC4979220
- DOI: 10.1016/S2213-8587(15)00225-9
Thyroid function in critically ill patients
Abstract
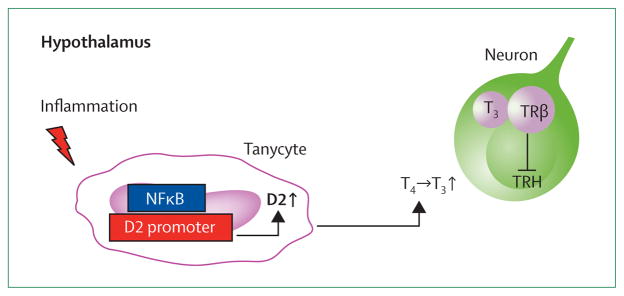
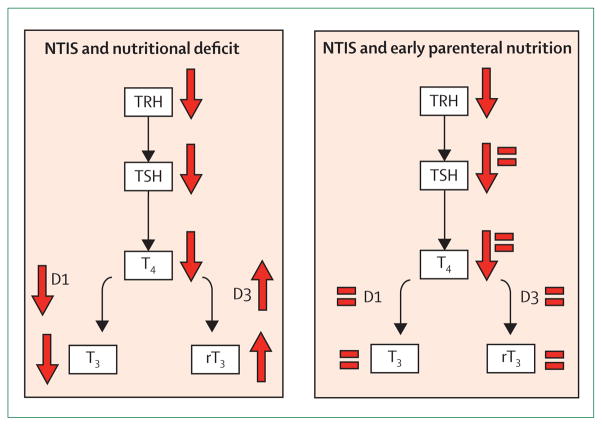
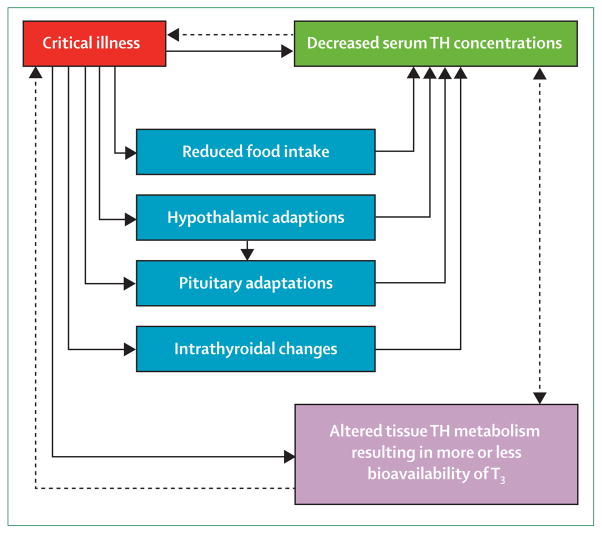
Patients in the intensive care unit (ICU) typically present with decreased concentrations of plasma tri-iodothyronine, low thyroxine, and normal range or slightly decreased concentration of thyroid-stimulating hormone. This ensemble of changes is collectively known as non-thyroidal illness syndrome (NTIS). The extent of NTIS is associated with prognosis, but no proof exists for causality of this association. Initially, NTIS is a consequence of the acute phase response to systemic illness and macronutrient restriction, which might be beneficial. Pathogenesis of NTIS in long-term critical illness is more complex and includes suppression of hypothalamic thyrotropin-releasing hormone, accounting for persistently reduced secretion of thyroid-stimulating hormone despite low plasma thyroid hormone. In some cases distinguishing between NTIS and severe hypothyroidism, which is a rare primary cause for admission to the ICU, can be difficult. Infusion of hypothalamic-releasing factors can reactivate the thyroid axis in patients with NTIS, inducing an anabolic response. Whether this approach has a clinical benefit in terms of outcome is unknown. In this Series paper, we discuss diagnostic aspects, pathogenesis, and implications of NTIS as well as its distinction from severe, primary thyroid disorders in patients in the ICU.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We declare no competing interests.
Figures
References
-
- Alkemade A, Friesema EC, Unmehopa UA, et al. Neuroanatomical pathways for thyroid hormone feedback in the human hypothalamus. J Clin Endocrinol Metab. 2005;90:4322–34. - PubMed
-
- Boelen A, Kwakkel J, Fliers E. Beyond low plasma T3: local thyroid hormone metabolism during inflammation and infection. Endocr Rev. 2011;32:670–93. - PubMed
-
- Wiersinga WM, van den Berghe G. Nonthyroidal illness syndrome. In: Braverman LE, Cooper DS, editors. Werner & Ingbar’s the thyroid: a fundamental and clinical text. 10. Philadelphia: Lippincott Williams and Wilkins; 2013. pp. 203–17.
-
- Wartofsky L, Burman KD. Alterations in thyroid function in patients with systemic illness: the “euthyroid sick syndrome”. Endocr Rev. 1982;3:164–217. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
