

Delivering an Optimised Behavioural Intervention (OBI) to people with low back pain with high psychological risk; results and lessons learnt from a feasibility randomised controlled trial of Contextual Cognitive Behavioural Therapy (CCBT) vs. Physiotherapy
- PMID: 26076755
- PMCID: PMC4468803
- DOI: 10.1186/s12891-015-0594-2
Delivering an Optimised Behavioural Intervention (OBI) to people with low back pain with high psychological risk; results and lessons learnt from a feasibility randomised controlled trial of Contextual Cognitive Behavioural Therapy (CCBT) vs. Physiotherapy
Abstract
Background: Low Back Pain (LBP) remains a common and costly problem. Psychological obstacles to recovery have been identified, but psychological and behavioural interventions have produced only moderate improvements. Reviews of trials have suggested that the interventions lack clear theoretical basis, are often compromised by low dose, lack of fidelity, and delivery by non-experts. In addition, interventions do not directly target known risk mechanisms. We identified a theory driven intervention (Contexual Cognitive Behavioural Therapy, CCBT) that directly targets an evidence-based risk mechanism (avoidance and ensured dose and delivery were optimised. This feasibility study was designed to test the credibility and acceptability of optimised CCBT against physiotherapy for avoidant LBP patients, and to test recruitment, delivery of the intervention and response rates prior to moving to a full definitive trial.
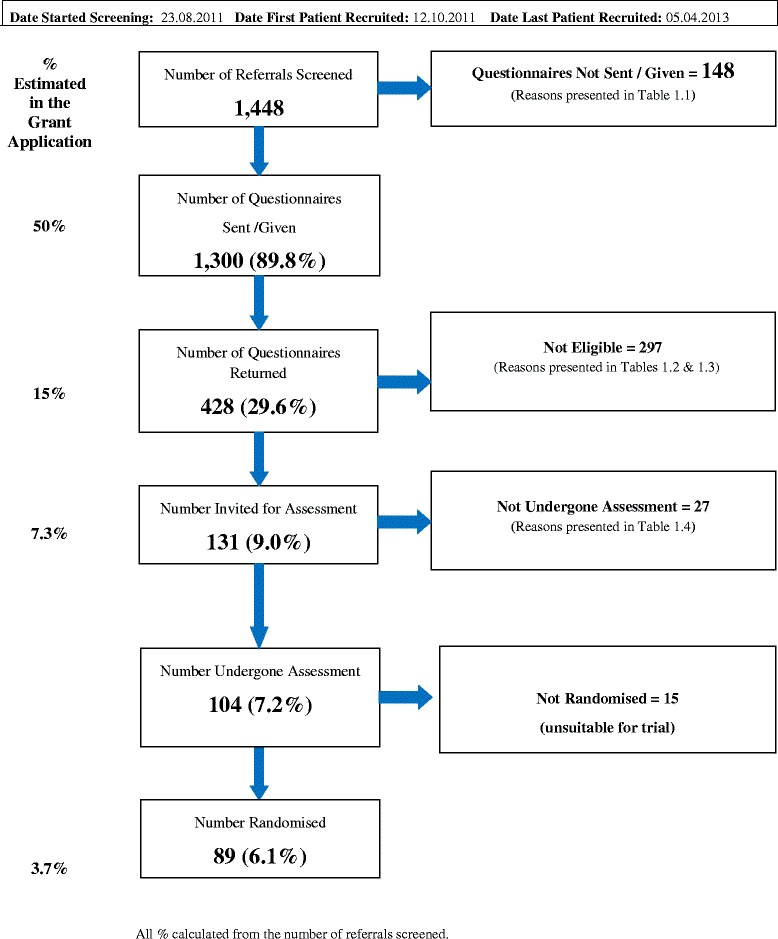
Methods: A randomised controlled feasibility trial with patients randomised to receive CCBT or physiotherapy. CCBT was delivered by trained supervised psychologists on a one to one basis and comprised up to 8 one-hour sessions. Physiotherapy comprised back to fitness group exercises with at least 60 % of content exercise-based. Patients were eligible to take part if they had back pain for more than 3 months, and scored above a threshold indicating fear avoidance, catastrophic beliefs and distress.
Results: 89 patients were recruited. Uptake rates were above those predicted. Scores for credibility and acceptability of the interventions met the set criteria. Response rates at three and six months fell short of the 75 % target. Problems associated with poor response rates were identified and successfully resolved, rates increased to 77 % at 3 months, and 68 % at 6 months. Independent ratings of treatment sessions indicated that CCBT was delivered to fidelity. Numbers were too small for formal analysis. Although average scores for acceptance were higher in the CCBT group than in the group attending physiotherapy (increase of 7.9 versus 5.1) and change in disability and pain from baseline to 6 months were greater in the CCBT group than in the physiotherapy group, these findings should be interpreted with caution.
Conclusions: CCBT is a credible and acceptable intervention for LBP patients who exhibit psychological obstacles to recovery.
Trial registration: ISRCTN43733490 , registered 15/12/2010.
Figures
References
-
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, Amann M, Anderson HR, Andrews KG, Aryee M, Atkinson C, Bacchus LJ, Bahalim AN, Balakrishnan K, Balmes J, Barker-Collo S, Baxter A, Bell ML, Blore JD, Blyth F, Bonner C, Borges G, Bourne R, Boussinesq M, Brauer M, Brooks P, Bruce NG, Brunekreef B, Bryan-Hancock C, Bucello C, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224–60. doi: 10.1016/S0140-6736(12)61766-8. - DOI - PMC - PubMed
-
- Eccleston C, Williams AC de C, Morley S: Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev 2009;2:CD007407. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
