

Risk factors and their interaction on chronic kidney disease: A multi-centre case control study in Taiwan
- PMID: 26077152
- PMCID: PMC4469431
- DOI: 10.1186/s12882-015-0065-x
Risk factors and their interaction on chronic kidney disease: A multi-centre case control study in Taiwan
Abstract
Background: Chronic kidney disease (CKD) is highly prevalent in Taiwan. More than two-thirds of end-stage renal disease is associated with diabetes mellitus (DM) or hypertension (HTN). Therefore, the formulation of a special preventative policy of CKD in these patients is essential. This study surveyed 14 traditional risk factors and identified their effects on CKD in patients with HTN/DM and compared these with their effects in the general population.
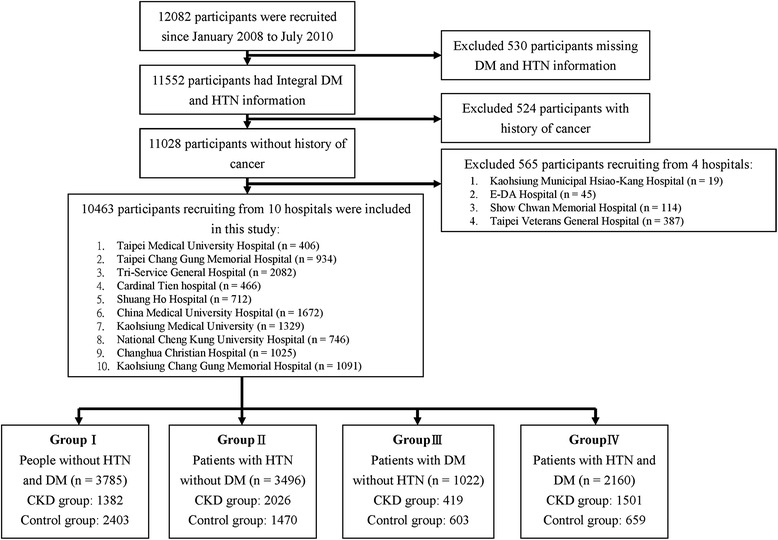
Methods: This study included 5328 cases and 5135 controls in the CKD/HTN/DM outpatient and health centres of 10 hospitals from 2008 to 2010. Fourteen common effect factors were surveyed (four demographic, five disease and five lifestyle), and their effects on CKD were tested. Significance tests were adjusted by the Bonferroni method. Results of the stratified analyses in the variables were presented with significant heterogeneity between patients with different comorbidities.
Results: Male, ageing, low income, hyperuricemia and lack of exercise habits were risk factors for CKD, and their effects in people with different comorbidities were identical. Anaemia was a risk factor, and there was an additive effect between anaemia and HTN on CKD. Patients with anaemia had a higher risk when associated with HTN [odds ratio (OR) = 6.75, 95% confidence limit (95% CI) 4.76-9.68] but had a smaller effect in people without HTN (OR 2.83, 95% CI 2.16-3.67). The association between hyperlipidaemia-related factors and CKD was also moderated by HTN. It was a significant risk factor in people without HTN (OR = 1.67, 95% CI 1.38-2.01) but not in patients with HTN (OR =1.03, 95% CI 0.89-1.19). Hepatitis B, hepatitis C, betel nut chewing, smoking, alcohol intake and groundwater use were not associated with CKD in multivariate analysis.
Conclusions: We considered that patients with HTN and anaemia were a high CKD risk population. Physicians with anaemic patients in outpatient clinics need to recognise that patients who also have HTN might be latent CKD cases.
Figures

References
-
- Bethesda MD. Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. U.S. Renal Data System, USRDS, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. 2013. http://www.usrds.org/2013/pdf/v2_ch12_13.pdf. Accessed November 12 2013.
-
- Li PK, Weening JJ, Dirks J, Lui SL, Szeto CC, Tang S et al. A report with consensus statements of the International Society of Nephrology 2004 Consensus Workshop on Prevention of Progression of Renal Disease, Hong Kong, June 29, 2004. Kidney international Supplement. 2005(94):S2-7. doi:10.1111/j.1523-1755.2005.09401.x. - PubMed
-
- Hallan SI, Dahl K, Oien CM, Grootendorst DC, Aasberg A, Holmen J et al. Screening strategies for chronic kidney disease in the general population: follow-up of cross sectional health survey. BMJ (Clinical research ed). 2006;333(7577):1047. doi:10.1136/bmj.39001.657755.BE. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
