

Comparison study of gastrinomas between gastric and non-gastric origins
- PMID: 26077245
- PMCID: PMC4478711
- DOI: 10.1186/s12957-015-0614-6
Comparison study of gastrinomas between gastric and non-gastric origins
Abstract
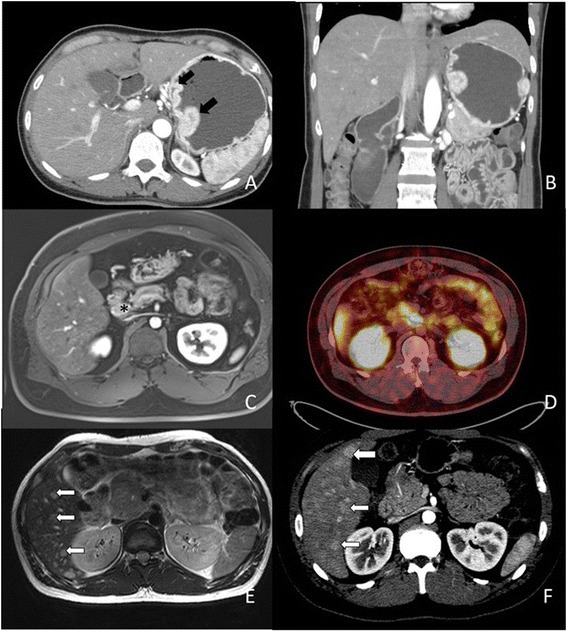
Background: Gastrinomas are one of the neuroendocrine tumors with potential distant metastasis. Most gastrinomas are originated from pancreas and duodenum, but those of gastric origin have been much less reported. The aim of the study is to compare gastrinomas of gastric and non-gastric origins.
Methods: Four hundred twenty-four patients with neuroendocrine tumor by histological proof in Chang Gung Memorial Hospital, Linkou branch in the past 10 years were included. A total of 109 (25.7 %) cases were identified of upper gastrointestinal origins, of which 20 (18.3 %) were proven gastrinomas. The clinical characteristics were collected and analyzed retrospectively.
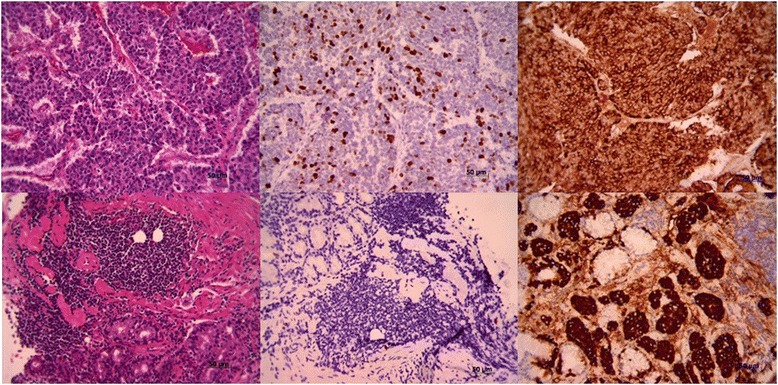
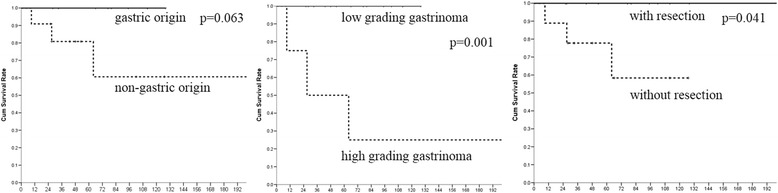
Results: In our study, 21 tumors of the 20 cases were identified by pathologic proof, 11 (55 %) had resection or endoscopic mucosa resection, 9 of gastric origins, 9 of duodenal origins, 2 of pancreatic origins, and 1 of hepatic origins. One case had multiple lesions. Patients with gastric gastrinomas had older age, higher levels of gastrin, seemingly smaller tumor size (p = 0.024, 0.030, and 0.065, respectively), and usually lower grade in differentiation (p = 0.035). Though gastric gastrinomas had a high recurrent rate (80 %), the lymph node and liver involvement was less common. Gastrinomas with liver involvement/metastasis had a high mortality rate where 80 % died of liver dysfunction.
Conclusions: Gastrinomas originating from stomach had higher gastrin level and lower tumor grading and presented at older age. The long-term outcome was probably better than non-gastric origin because of lower grading and less lymph node and liver involvement.
Figures
References
-
- Garcia-Carbonero R, Capdevila J, Crespo-Herrero G, Diaz-Perez JA, Martinez Del Prado MP, Alonso Orduna V, et al. Incidence, patterns of care and prognostic factors for outcome of gastroenteropancreatic neuroendocrine tumors (GEP-NETs): results from the National Cancer Registry of Spain (RGETNE) Ann Oncol. 2010;21(9):1794–803. doi: 10.1093/annonc/mdq022. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
