

Differentiation of infiltrative cardiomyopathy from hypertrophic cardiomyopathy using high-sensitivity cardiac troponin T: a case-control study
- PMID: 26077897
- PMCID: PMC4467071
- DOI: 10.1186/s12872-015-0043-z
Differentiation of infiltrative cardiomyopathy from hypertrophic cardiomyopathy using high-sensitivity cardiac troponin T: a case-control study
Abstract
Background: Because infiltrative cardiomyopathy and hypertrophic cardiomyopathy (HCM) share clinical and hemodynamic features of left ventricular (LV) hypertrophy and abnormal diastolic function, it is often difficult to distinguish these entities.
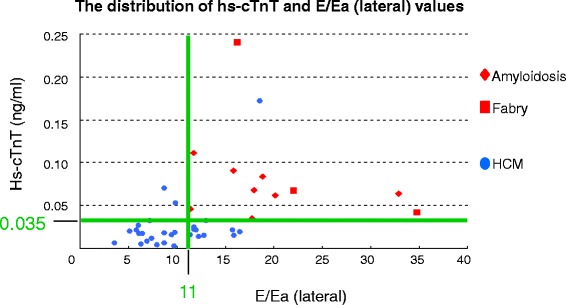
Methods: We investigated the potential role of high-sensitivity cardiac troponin T (hs-cTnT) for differentiation of infiltrative cardiomyopathy from HCM.
Results: The study group consisted of 46 consecutive patients with infiltrative cardiomyopathies or HCM in whom sarcomere protein gene mutations were identified at Kochi Medical School Hospital; of these, there were 11 patients with infiltrative cardiomyopathy (cardiac amyloidosis in 8 patients and Fabry disease in 3 patients) and 35 HCM patients. Serum hs-cTnT level was significantly higher in patients who had infiltrative cardiomyopathy than in those who had HCM (0.083 ± 0.057 ng/ml versus 0.027 ± 0.034 ng/ml, p < 0.001), whereas brain natriuretic peptide levels did not differ between the two groups. In two age-matched the 2 cohorts (patients evaluated at > 40 years at age), hs-cTnT level, maximum LV wall thickness, posterior wall thickness, peak early (E) transmitral filling velocity, peak early diastolic (Ea) velocity of tissue Doppler imaging at the lateral corner and E/Ea ratios at both the septal and lateral corners were significantly different between the two groups. As for diagnostic accuracy to differentiate the two groups by using receiver operating characteristic analysis, hs-cTnT was the highest value of area under the curve (0.939) and E/Ea (lateral) was second highest value (0.914).
Conclusions: Serum hs-cTnT is a helpful diagnostic indicator for accurate differentiation between infiltrative cardiomyopathy and HCM.
Figures


Similar articles
-
Prevalence and determinants of elevated high-sensitivity cardiac troponin T in hypertrophic cardiomyopathy.J Cardiol. 2014 Feb;63(2):140-4. doi: 10.1016/j.jjcc.2013.07.008. Epub 2013 Sep 4. J Cardiol. 2014. PMID: 24011925
-
Serum cardiac troponin I is related to increased left ventricular wall thickness, left ventricular dysfunction, and male gender in hypertrophic cardiomyopathy.Clin Cardiol. 2010 Feb;33(2):E1-7. doi: 10.1002/clc.20622. Clin Cardiol. 2010. PMID: 20043329 Free PMC article.
-
Significance of high-sensitivity cardiac troponin T in hypertrophic cardiomyopathy.J Am Coll Cardiol. 2013 Oct 1;62(14):1252-1259. doi: 10.1016/j.jacc.2013.03.055. Epub 2013 Apr 23. J Am Coll Cardiol. 2013. PMID: 23623916
-
Common presentation of rare diseases: Left ventricular hypertrophy and diastolic dysfunction.Int J Cardiol. 2018 Apr 15;257:344-350. doi: 10.1016/j.ijcard.2018.01.006. Int J Cardiol. 2018. PMID: 29506729 Review.
-
Tissue Doppler imaging in Fabry disease.Curr Opin Cardiol. 2004 Sep;19(5):452-7. doi: 10.1097/01.hco.0000131534.25034.43. Curr Opin Cardiol. 2004. PMID: 15316452 Review.
Cited by
-
Diagnostic utility of cardiac troponin T level in patients with cardiac amyloidosis.ESC Heart Fail. 2018 Feb;5(1):27-35. doi: 10.1002/ehf2.12203. Epub 2017 Sep 4. ESC Heart Fail. 2018. PMID: 28869340 Free PMC article.
-
Positive Myocardial Uptake of Bone Scintigraphic Agents Associated with Cardiac Amyloidosis: Frequency of Positive Uptake Data Based on Daily Clinical Practice.Ann Nucl Cardiol. 2020;6(1):27-32. doi: 10.17996/anc.20-00121. Epub 2020 Aug 31. Ann Nucl Cardiol. 2020. PMID: 37123498 Free PMC article.
-
Value of cardiac biomarker measurement in the differential diagnosis of infiltrative cardiomyopathy patients with preserved left ventricular systolic function.J Thorac Dis. 2018 Aug;10(8):4966-4975. doi: 10.21037/jtd.2018.07.56. J Thorac Dis. 2018. PMID: 30233871 Free PMC article.
-
Biomarkers and Imaging Findings of Anderson-Fabry Disease-What We Know Now.Diseases. 2017 Jun 11;5(2):15. doi: 10.3390/diseases5020015. Diseases. 2017. PMID: 28933368 Free PMC article. Review.
-
Coronary arterial vasculature in the pathophysiology of hypertrophic cardiomyopathy.Pflugers Arch. 2019 May;471(5):769-780. doi: 10.1007/s00424-018-2224-y. Epub 2018 Oct 29. Pflugers Arch. 2019. PMID: 30370501 Free PMC article. Review.
References
-
- Cueto-Garcia L, Reeder GS, Kyle RA, Wood DL, Seward JB, Naessens J, Offorrd KP, Greipp PR, Edwards WD, Tajik AJ. Echocardiographic findings in systemic amyloidosis: spectrum of cardiac involvement and relation to survival. J Am Coll Cardiol. 1985;6:737–43. doi: 10.1016/S0735-1097(85)80475-7. - DOI - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
