

Review of diagnostic and therapeutic endoscopic retrograde cholangiopancreatography using several endoscopic methods in patients with surgically altered gastrointestinal anatomy
- PMID: 26078830
- PMCID: PMC4461936
- DOI: 10.4253/wjge.v7.i6.617
Review of diagnostic and therapeutic endoscopic retrograde cholangiopancreatography using several endoscopic methods in patients with surgically altered gastrointestinal anatomy
Abstract
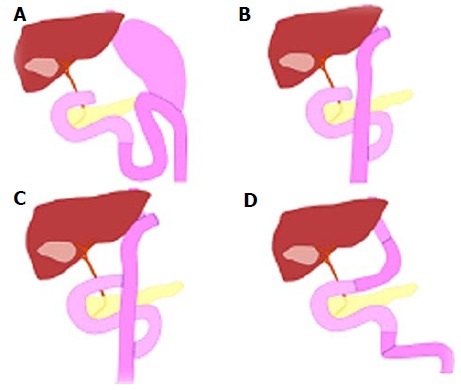
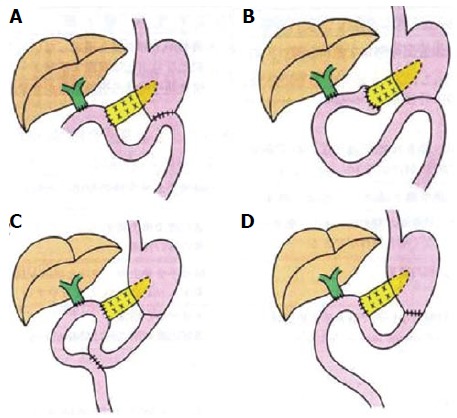
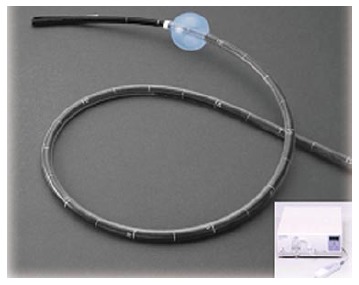
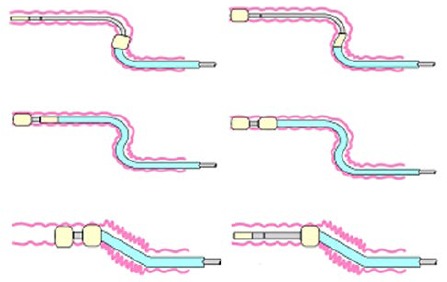
The endoscopic approach for biliary diseases in patients with surgically altered gastrointestinal anatomy (SAGA) had been generally deemed impractical. However, it was radically made feasible by the introduction of double balloon endoscopy (DBE) that was originally developed for diagnosis and treatments for small-bowel diseases. Followed by the subsequent development of single-balloon endoscopy (SBE) and spiral endoscopy (SE), interventions using several endoscopes for biliary disease in patients with SAGA widely gained an acceptance as a new modality. Many studies have been made on this new technique. Yet, some problems are to be solved. For instance, the mutual unavailability among devices due to different working lengths and channels, and unestablished standardization of procedural techniques can be raised. Additionally, in an attempt to standardize endoscopic procedures, it is important to evaluate biliary cannulating methods by case with existence of papilla or not. A full comprehension of the features of respective scope types is also required. However there are not many papers written as a review. In our manuscript, we would like to evaluate and make a review of the present status of diagnostic and therapeutic endoscopic retrograde cholangiopancreatography applying DBE, SBE and SE for biliary diseases in patients with SAGA for establishment of these modalities as a new technology and further improvement of the scopes and devices.
Keywords: Double balloon endoscopy; Endoscopic retrograde cholangiopancreatography; Roux-en-Y reconstruction; Single balloon endoscopy; Spiral endoscopy.
Figures


References
-
- Suissa A, Yassin K, Lavy A, Lachter J, Chermech I, Karban A, Tamir A, Eliakim R. Outcome and early complications of ERCP: a prospective single center study. Hepatogastroenterology. 2005;52:352–355. - PubMed
-
- Freeman ML, Guda NM. ERCP cannulation: a review of reported techniques. Gastrointest Endosc. 2005;61:112–125. - PubMed
-
- Maaser C, Lenze F, Bokemeyer M, Ullerich H, Domagk D, Bruewer M, Luegering A, Domschke W, Kucharzik T. Double balloon enteroscopy: a useful tool for diagnostic and therapeutic procedures in the pancreaticobiliary system. Am J Gastroenterol. 2008;103:894–900. - PubMed
-
- Teplick SK, Flick P, Brandon JC. Transhepatic cholangiography in patients with suspected biliary disease and nondilated intrahepatic bile ducts. Gastrointest Radiol. 1991;16:193–197. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
