

Diagnosis and management of lentigo maligna: a review
- PMID: 26082796
- PMCID: PMC4453766
- DOI: 10.7573/dic.212281
Diagnosis and management of lentigo maligna: a review
Abstract
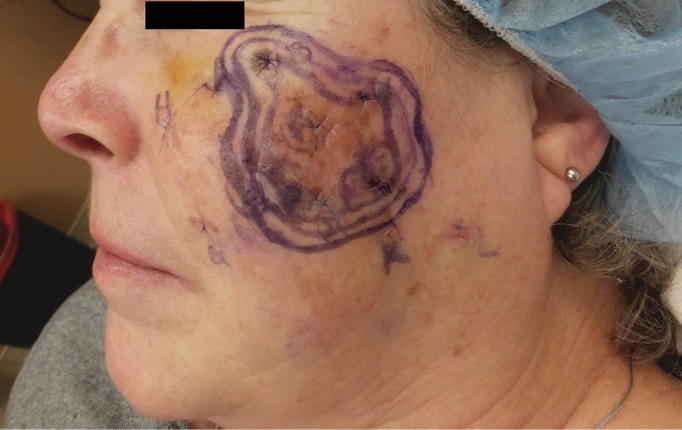
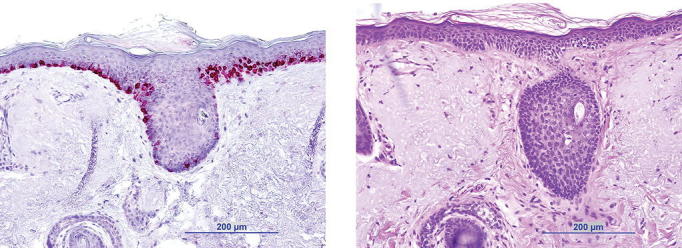
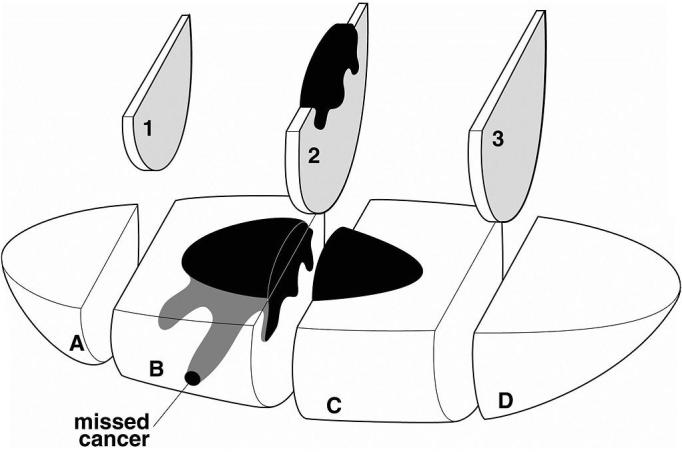
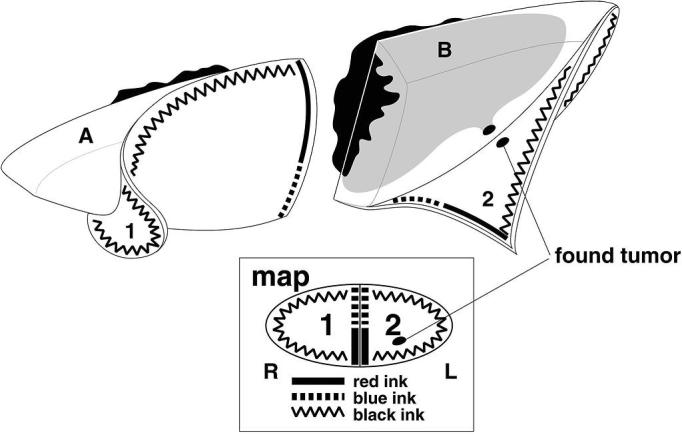
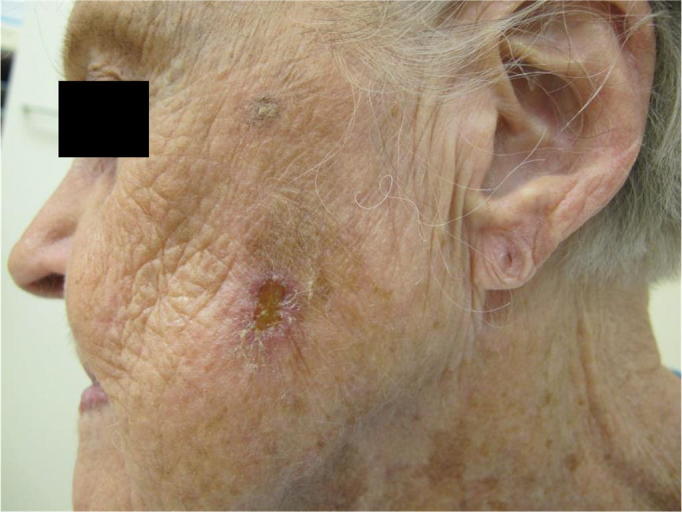
Lentigo maligna is a melanocytic neoplasm occurring on sun-exposed skin, usually on the head and neck, of middle-aged and elderly patients. It is thought to represent the in situ phase of lentigo maligna melanoma. The ill-defined nature and potentially large size of lesions can pose significant diagnostic and treatment challenges. The goal of therapy is to cure the lesions in order to prevent development of invasive disease, and surgical excision is the treatment of choice to achieve clear histological margins. Nonsurgical treatment modalities have been reported; however, evidence is lacking to support their use. Age, general health, and comorbidities need to be taken into account when deciding the right treatment modality for each individual patient.
Keywords: Mohs micrographic surgery; diagnosis; histopathology; imiquimod; immunohistochemistry; lentigo maligna; staged excision.
Figures








References
-
- van Ruth S, Toonstra J. Eponyms of Sir Jonathan Hutchinson. Int J Dermatol. 2008;47(7):754–8. http://dx.doi.org/10.1111/j.1365-4632.2008.03696.x. - DOI - PubMed
-
- Gaudy-Marqueste C, Madjlessi N, Guillot B, Avril MF, Grob JJ. Risk factors in elderly people for lentigo maligna compared with other melanomas: a double case-control study. Arch Dermatol. 2009;145(4):418–23. http://dx.doi.org/10.1001/archdermatol.2009.1. - DOI - PubMed
-
- Purdue MP, From L, Kahn HJ, Armstrong BK, Kricker A, Gallagher RP, McLaughlin JR, Klar NS, Marrett LD. Etiologic factors associated with p53 immunostaining in cutaneousmalignant melanoma. Int J Cancer. 2005;117(3):486–93. http://dx.doi.org/10.1002/ijc.21196. - DOI - PubMed
-
- Sasaki Y, Niu C, Makino R, Kudo C, Sun C, Watanabe H, Matsunaga J, Takahashi K, Tagami H, Aiba S, Horii A. BRAF point mutations in primary melanoma show different prevalences by subtype. J Invest Dermatol. 2004;123(1):177–83. http://dx.doi.org/10.1111/j.0022-202X.2004.22722.x. - DOI - PubMed
-
- Maldonado JL, Fridlyand J, Patel H, Jain AN, Busam K, Kageshita T, Ono T, Albertson DG, Pinkel D, Bastian BC. Determinants of BRAF mutations in primary melanomas. J Natl Cancer Inst. 2003;95(24):1878–90. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
