

Semi-quantitative contrast-enhanced MR analysis of indeterminate ovarian tumours: when to say malignancy?
- PMID: 26083260
- PMCID: PMC4743568
- DOI: 10.1259/bjr.20150099
Semi-quantitative contrast-enhanced MR analysis of indeterminate ovarian tumours: when to say malignancy?
Abstract
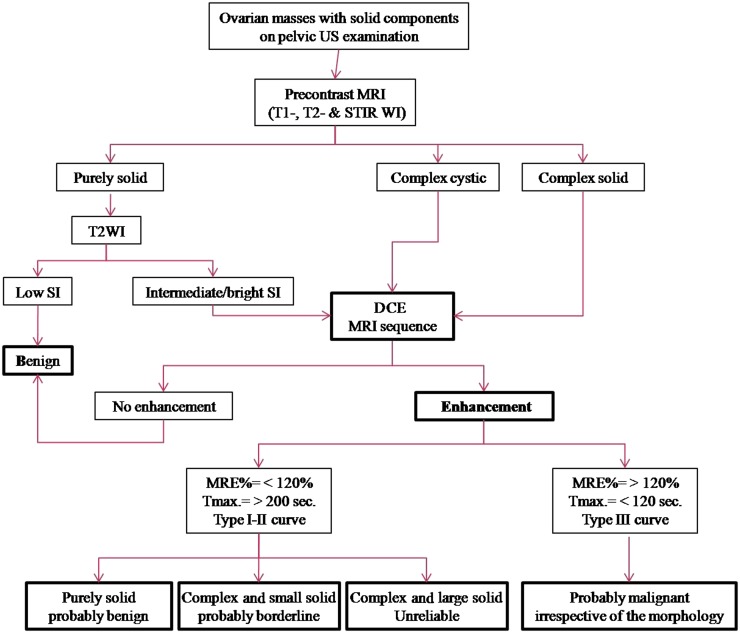
Objective: To evaluate the ability of dynamic post-contrast sequence to specify indeterminate ovarian masses with inconclusive MR features of malignancy. Since management is dramatically different, special focus on the ability to differentiate borderline from invasive malignancy was considered.
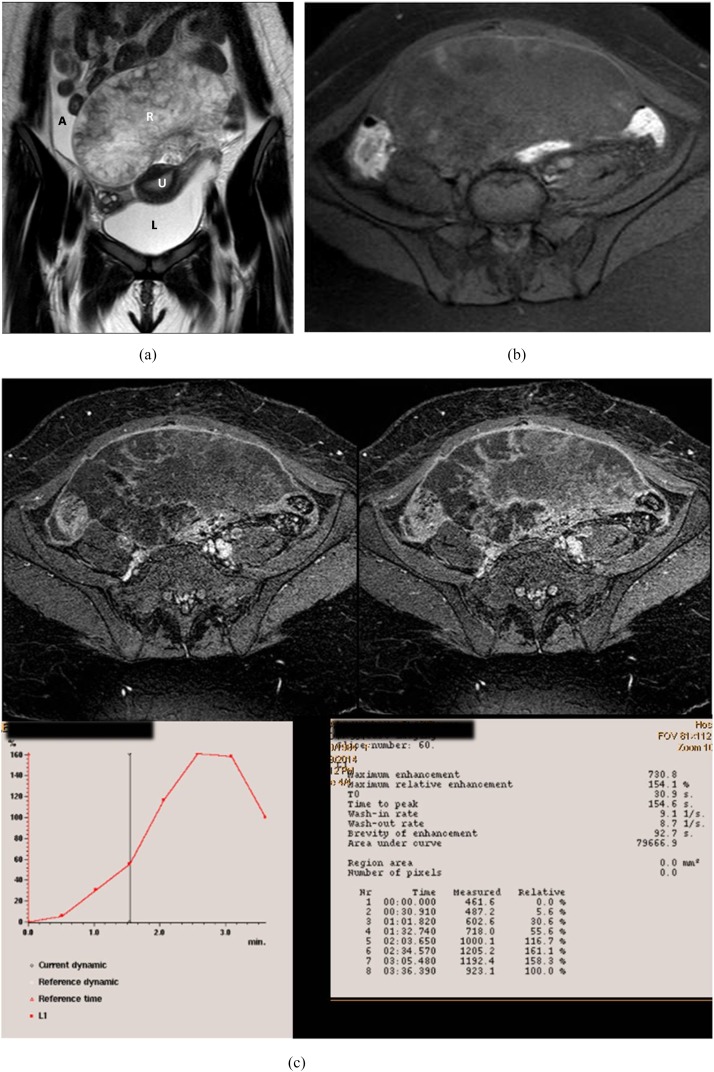
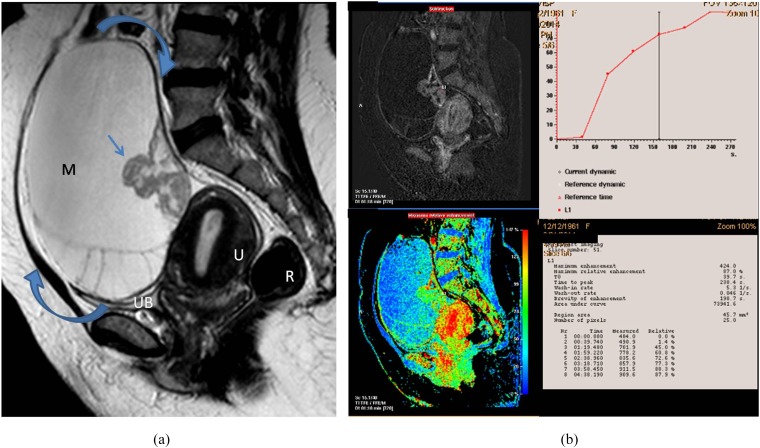
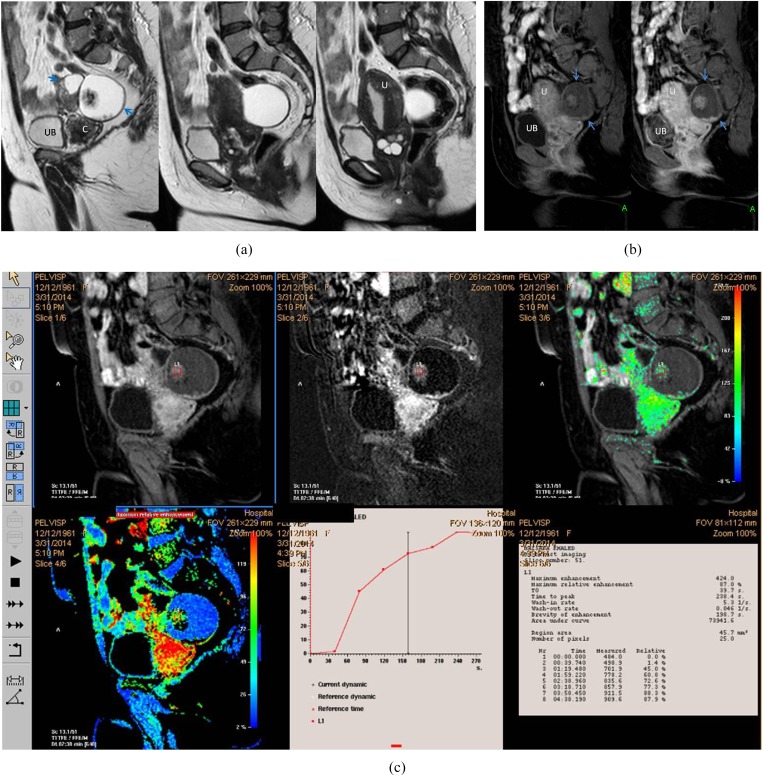
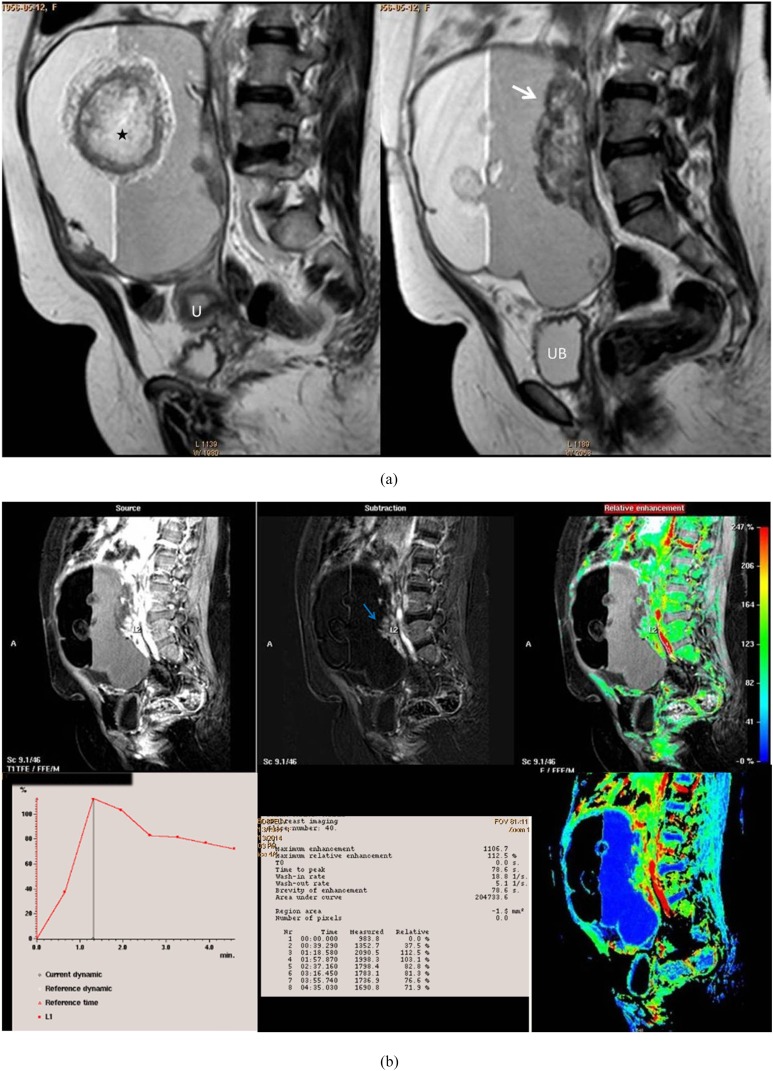
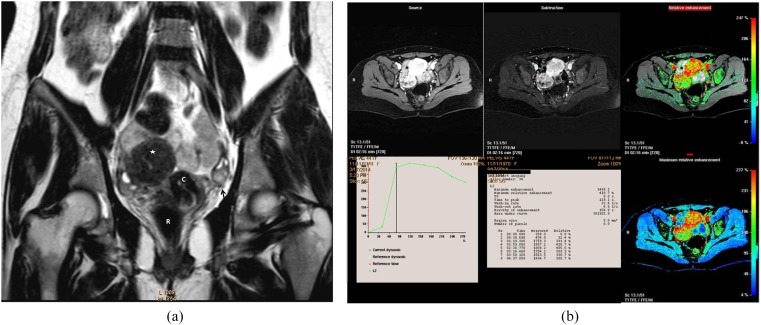
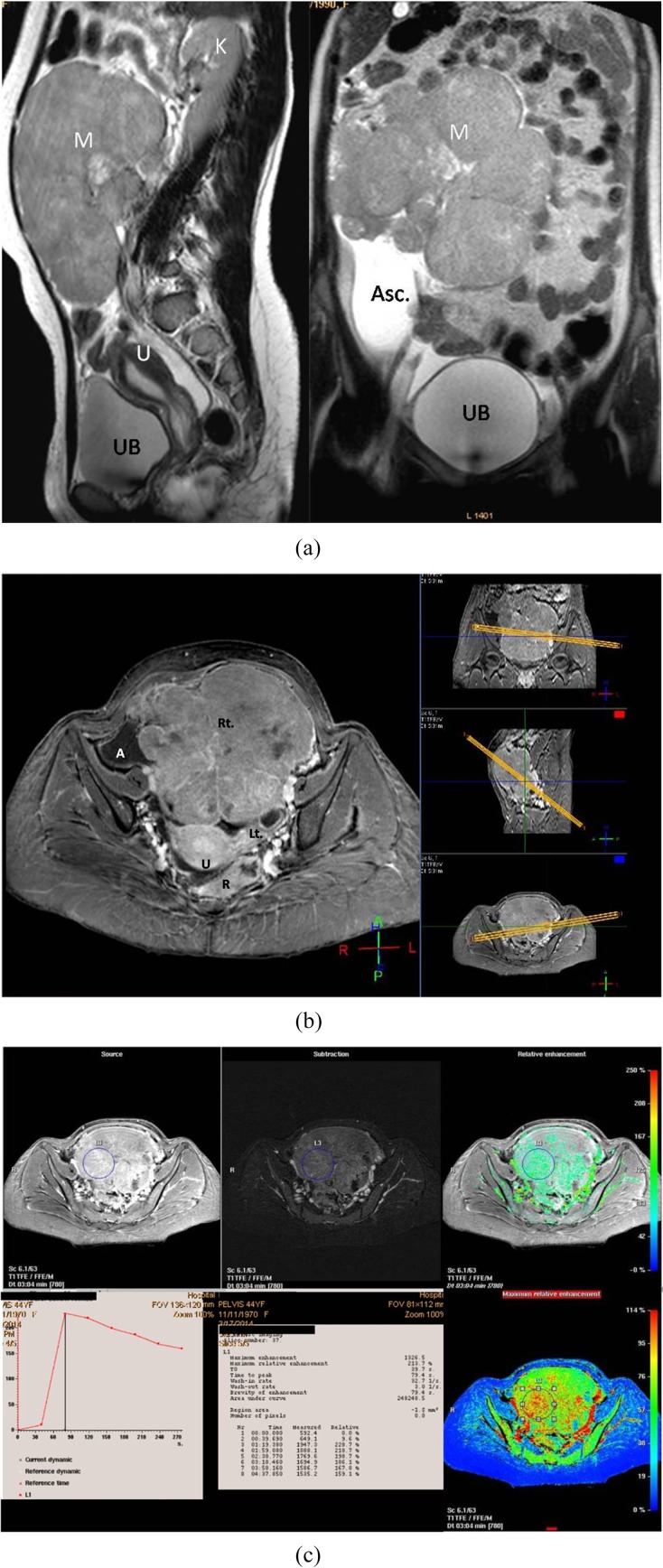
Methods: 150 ovarian masses were detected by pelvic ultrasound in 124 patients. Masses had been considered for dynamic post-contrast MRI. We expressed the kinetic parameters (i.e. enhancement amplitude, time peak of maximal uptake and maximal slope) in the form of maximum relative enhancement percentage (MRE%), time of maximal peak of contrast uptake (Tmax) and slope enhancement ratio (SER) curves. Histological findings were the gold standard of reference.
Results: Malignant ovarian masses showed higher MRE% than benign and borderline masses (p < 0.001). Tmax was shorter for malignant than benign (p < 0.01) and borderline (p < 0.001) ovarian masses. SER curves were the most suggestive of malignancy with a specificity and accuracy of 85.7% and 84.7%, respectively.
Conclusion: Dynamic contrast-enhanced MRI could be a specific sequence to differentiate ovarian masses with indeterminate MR morphology with a special discrimination for low potential from invasive ovarian malignancy.
Advances in knowledge: The study evaluated the diagnostic performance of the individual parameters of dynamic post-contrast MR sequence in evaluating ovarian masses. Management divert between benign, borderline and invasive malignant masses; our work presented a cut-off value for the peak of contrast uptake of 120%, which helped in the differentiation between benign and malignant tumours; the SER curves with Type III (early washout) pattern that was indicative of invasive malignancy was more specific than borderline malignancy.
Figures
References
-
- Berek JS, Hacker NF. Practical gynecologic oncology. 4th edn. Philadelphia, PA: Lippincott Williams & Wilkins; 2005. pp. 443–54.
-
- Berek JS, Hacker NF. Staging and second-look operations in ovarian cancer. In: Alberts DS, Surwit EA, eds. Ovarian cancer. Boston, MA: Martinus Nijhoff; 1985. pp. 109–27.
-
- Gupta N, Rajpal T, Sharma S. Evaluating the accuracy of frozen section in borderline ovarian tumours. J Clin Oncol 2013; 31(Suppl.): Abstract 5564.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
