

Metabolic Effects of Exercise Training Among Fitness-Nonresponsive Patients With Type 2 Diabetes: The HART-D Study
- PMID: 26084342
- PMCID: PMC4512133
- DOI: 10.2337/dc14-2378
Metabolic Effects of Exercise Training Among Fitness-Nonresponsive Patients With Type 2 Diabetes: The HART-D Study
Abstract
Objective: To evaluate the impact of exercise training (ET) on metabolic parameters among participants with type 2 diabetes mellitus (T2DM) who do not improve their cardiorespiratory fitness (CRF) with training.
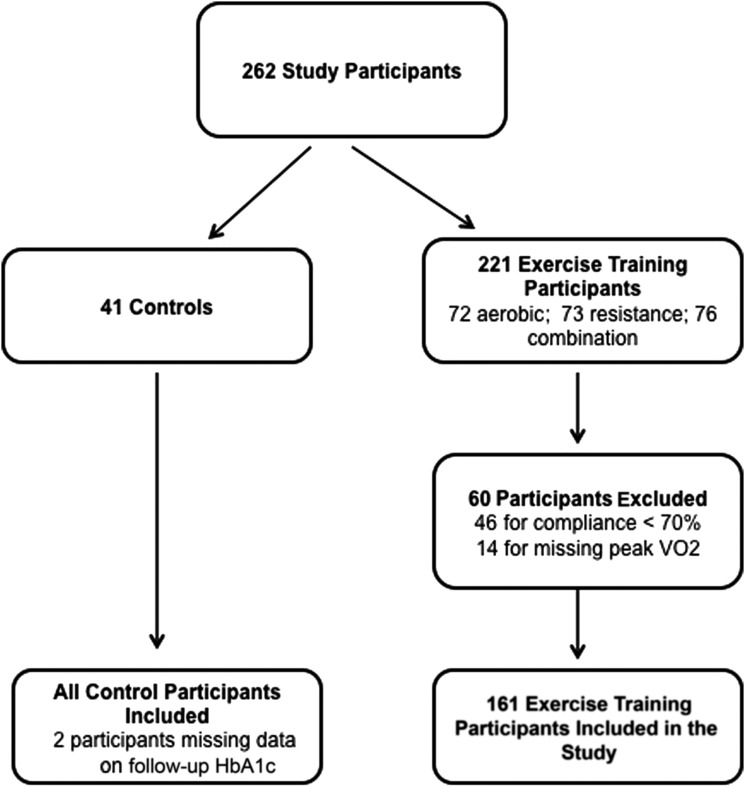
Research design and methods: We studied participants with T2DM participating in the Health Benefits of Aerobic and Resistance Training in Individuals With Type 2 Diabetes (HART-D) trial who were randomized to a control group or one of three supervised ET groups for 9 months. Fitness response to ET was defined as a change in measured peak absolute oxygen uptake (ΔVO(2peak), in liters per minute) from baseline to follow-up. ET participants were classified based on ΔVO(2peak) into fitness responders (ΔVO(2peak) ≥5%) and nonresponders (ΔVO(2peak) <5%), and changes in metabolic profiles were compared across control, fitness responder, and fitness nonresponder groups.
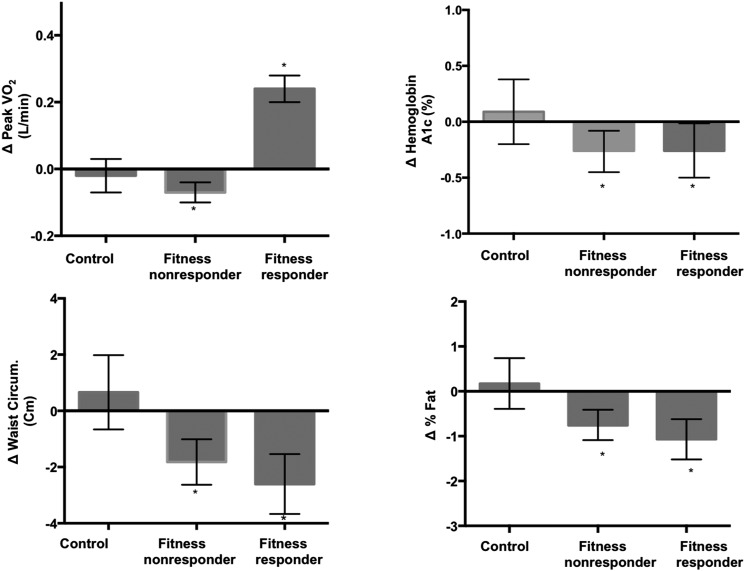
Results: A total of 202 participants (mean age 57.1 ± 7.9 years, 63% women) were included. Among the exercise groups (n = 161), there was substantial heterogeneity in ΔVO(2peak); 57% had some improvement in CRF (ΔVO(2peak) >0), with only 36.6% having a ≥5% increase in VO(2peak). Both fitness responders and nonresponders (respectively) had significant improvements in hemoglobin A1c and measures of adiposity (ΔHbA(1c): -0.26% [95% CI -0.5 to -0.01] and -0.26% [-0.45 to -0.08]; Δwaist circumference: -2.6 cm [-3.7 to -1.5] and -1.8 cm [-2.6 to -1.0]; Δbody fat: -1.07% [-1.5 to -0.62] and -0.75% [-1.09 to -0.41]). No significant differences were observed in the degree of change of these metabolic parameters between fitness responders and nonresponders. Control group participants had no significant changes in any of these metabolic parameters.
Conclusions: ET is associated with significant improvements in metabolic parameters irrespective of improvement in cardiorespiratory fitness.
Trial registration: ClinicalTrials.gov NCT00458133.
© 2015 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures

References
-
- Church TS, LaMonte MJ, Barlow CE, Blair SN. Cardiorespiratory fitness and body mass index as predictors of cardiovascular disease mortality among men with diabetes. Arch Intern Med 2005;165:2114–2120 - PubMed
-
- Snowling NJ, Hopkins WG. Effects of different modes of exercise training on glucose control and risk factors for complications in type 2 diabetic patients: a meta-analysis. Diabetes Care 2006;29:2518–2527 - PubMed
-
- Bouchard C, An P, Rice T, et al. Familial aggregation of VO(2max) response to exercise training: results from the HERITAGE Family Study. J Appl Physiol (1985) 1999;87:1003–1008 - PubMed
-
- Hautala AJ, Kiviniemi AM, Mäkikallio TH, et al. Individual differences in the responses to endurance and resistance training. Eur J Appl Physiol 2006;96:535–542 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
