

Comparison of effects of sitagliptin and voglibose on left ventricular diastolic dysfunction in patients with type 2 diabetes: results of the 3D trial
- PMID: 26084668
- PMCID: PMC4473835
- DOI: 10.1186/s12933-015-0242-z
Comparison of effects of sitagliptin and voglibose on left ventricular diastolic dysfunction in patients with type 2 diabetes: results of the 3D trial
Abstract
Background: Left ventricular (LV) diastolic dysfunction is frequently observed in patients with type 2 diabetes. Dipeptidyl peptidase-4 inhibitor (DPP-4i) attenuates postprandial hyperglycemia (PPH) and may have cardio-protective effects. It remains unclear whether DPP-4i improves LV diastolic function in patients with type 2 diabetes, and, if so, it is attributable to the attenuation of PPH or to a direct cardiac effect of DPP-4i. We compared the effects of the DPP-4i, sitagliptin, and the alpha-glucosidase inhibitor, voglibose, on LV diastolic function in patients with type 2 diabetes.
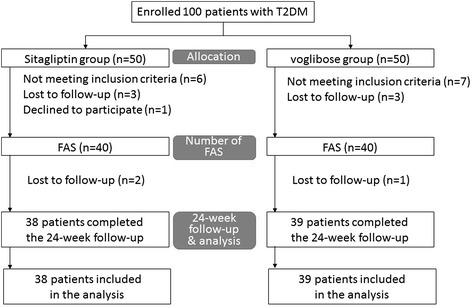
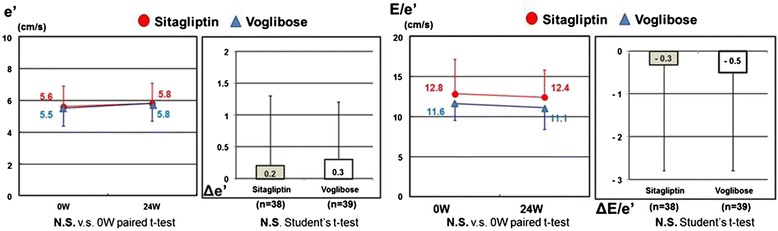
Methods: We conducted a prospective, randomized, open-label, multicenter study of 100 diabetic patients with LV diastolic dysfunction. Patients received sitagliptin (50 mg/day) or voglibose (0.6 mg/day). The primary endpoints were changes in the e' velocity and E/e' ratio from baseline to 24 weeks later. The secondary efficacy measures included HbA1c, GLP-1, lipid profiles, oxidative stress markers and inflammatory markers.
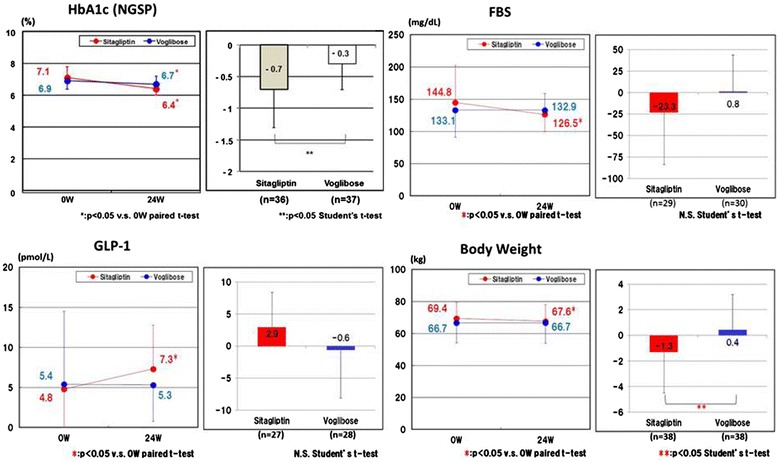
Results: The study was completed with 40 patients in the sitagliptin group and 40 patients in the voglibose group. There were no significant changes in the e' velocity and E/e' ratio from baseline to 24 weeks later in both groups. However, analysis of covariance demonstrated that pioglitazone use is an independent factor associated with changes in the e' and E/e' ratio. Among patients not using pioglitazone, e' increased and the E/e' ratio decreased in both the sitagliptin and voglibose groups. GLP-1 level increased from baseline to 24 weeks later only in the sitagliptin group (4.8 ± 4.7 vs. 7.3 ± 5.5 pmol/L, p < 0.05). The reductions in HbA1c and body weight were significantly greater in the sitagliptin group than in the voglibose group (-0.7 ± 0.6 % vs. -0.3 ± 0.4, p < 0.005; -1.3 ± 3.2 kg vs. 0.4 ± 2.8 kg, p < 0.05, respectively). There were no changes in lipid profiles and inflammatory markers in both groups.
Conclusions: Our trial showed that sitagliptin reduces HbA1c levels more greatly than voglibose does, but that neither was associated with improvement in the echocardiographic parameters of LV diastolic function in patients with diabetes.
Trial registration: Registered at http://www.umin.ac.jp under UMIN000003784.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
