

Successful mLearning Pilot in Senegal: Delivering Family Planning Refresher Training Using Interactive Voice Response and SMS
- PMID: 26085026
- PMCID: PMC4476867
- DOI: 10.9745/GHSP-D-14-00220
Successful mLearning Pilot in Senegal: Delivering Family Planning Refresher Training Using Interactive Voice Response and SMS
Abstract
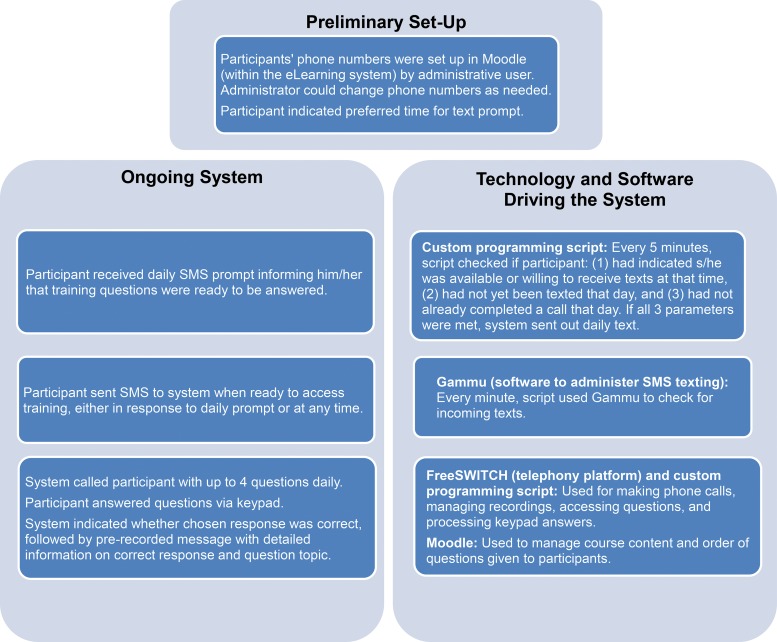
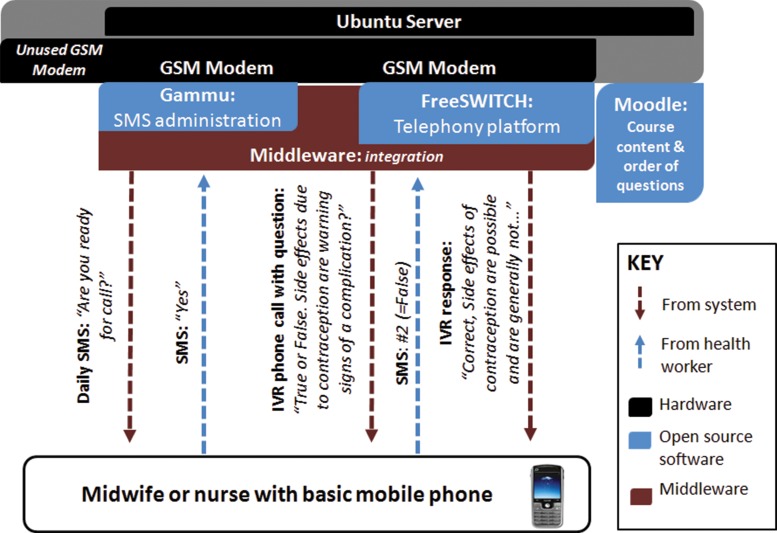
Background: In-service training of health workers plays a pivotal role in improving service quality. However, it is often expensive and requires providers to leave their posts. We developed and assessed a prototype mLearning system that used interactive voice response (IVR) and text messaging on simple mobile phones to provide in-service training without interrupting health services. IVR allows trainees to respond to audio recordings using their telephone keypad.
Methods: In 2013, the CapacityPlus project tested the mobile delivery of an 8-week refresher training course on management of contraceptive side effects and misconceptions to 20 public-sector nurses and midwives working in Mékhé and Tivaouane districts in the Thiès region of Senegal. The course used a spaced-education approach in which questions and detailed explanations are spaced and repeated over time. We assessed the feasibility through the system's administrative data, examined participants' experiences using an endline survey, and employed a pre- and post-test survey to assess changes in provider knowledge.
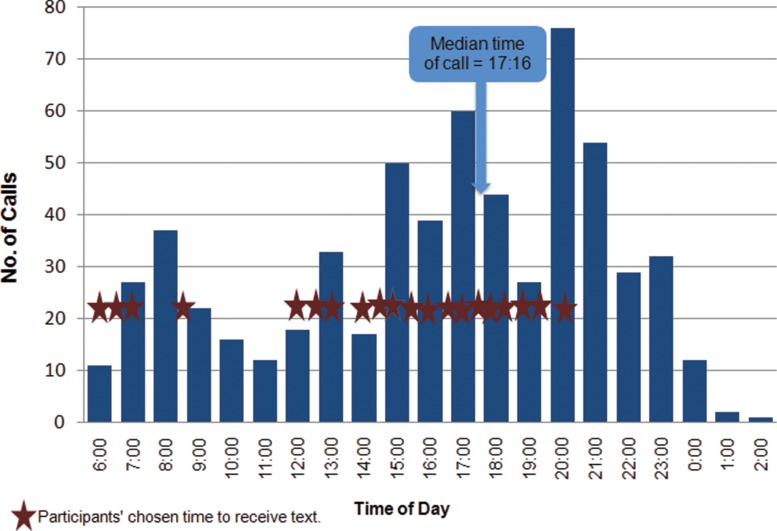
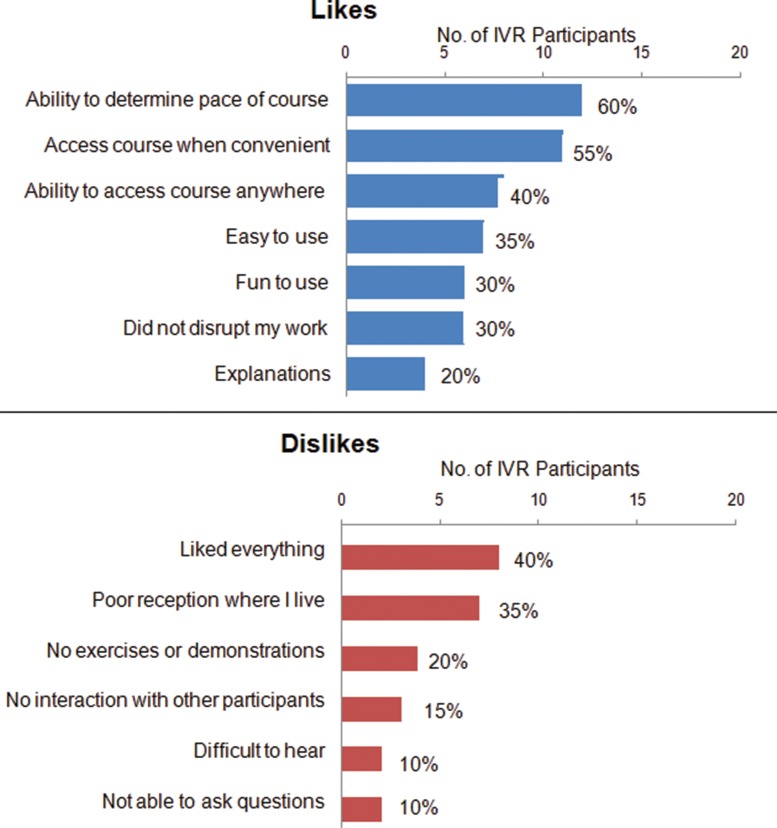
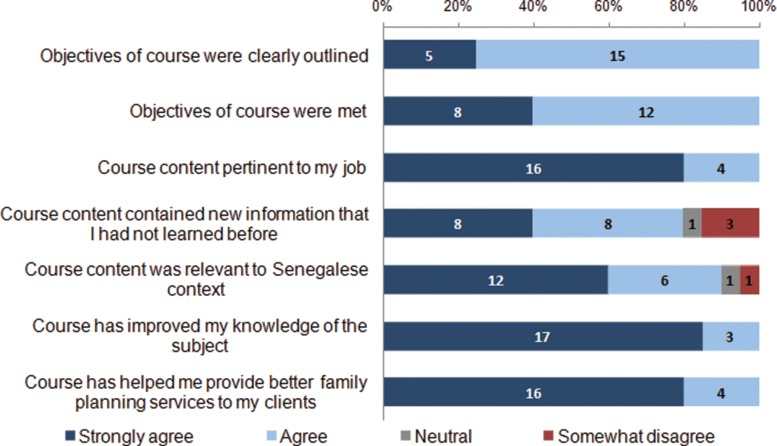
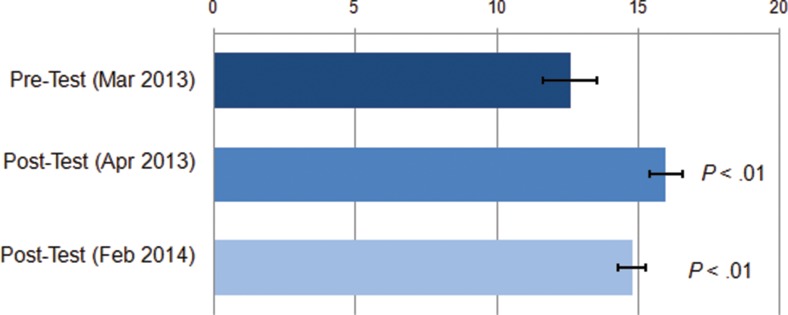
Results: All participants completed the course within 9 weeks. The majority of participant prompts to interact with the mobile course were made outside normal working hours (median time, 5:16 pm); average call duration was about 13 minutes. Participants reported positive experiences: 60% liked the ability to determine the pace of the course and 55% liked the convenience. The largest criticism (35% of participants) was poor network reception, and 30% reported dropped IVR calls. Most (90%) participants thought they learned the same or more compared with a conventional course. Knowledge of contraceptive side effects increased significantly, from an average of 12.6/20 questions correct before training to 16.0/20 after, and remained significantly higher 10 months after the end of training than at baseline, at 14.8/20, without any further reinforcement.
Conclusions: The mLearning system proved appropriate, feasible, and acceptable to trainees, and it was associated with sustained knowledge gains. IVR mLearning has potential to improve quality of care without disrupting routine service delivery. Monitoring and evaluation of larger-scale implementation could provide evidence of system effectiveness at scale.
© Diedhiou et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly cited. To view a copy of the license, visit http://creativecommons.org/licenses/by/3.0/
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous