

Autoregulation monitoring and outcome prediction in neurocritical care patients: Does one index fit all?
- PMID: 26085437
- PMCID: PMC4854943
- DOI: 10.1007/s10877-015-9726-3
Autoregulation monitoring and outcome prediction in neurocritical care patients: Does one index fit all?
Abstract
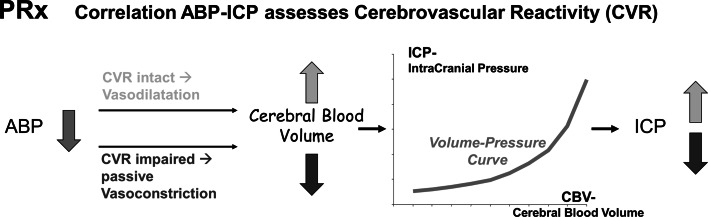
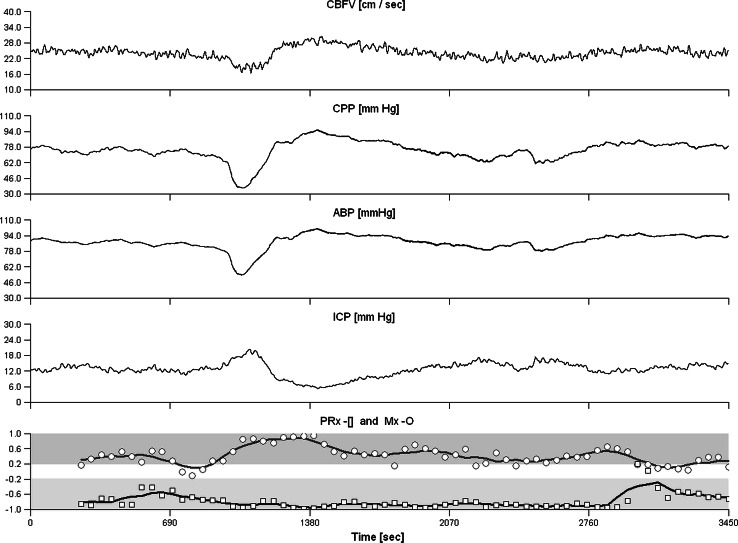
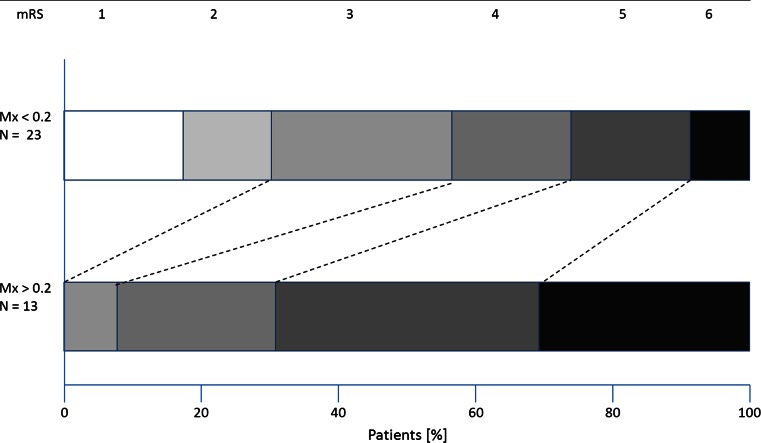
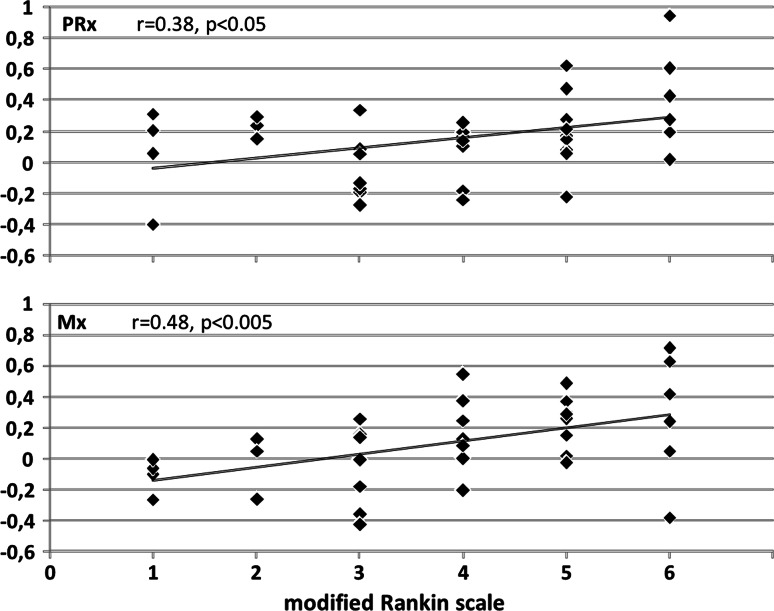
Indexes PRx and Mx have been formerly introduced to assess cerebral autoregulation and have been shown to be associated with 3-month clinical outcome. In a mixed cohort of neurocritical care patients, we retrospectively investigated the impact of selected clinical characteristics on this association. Forty-one patients (18-77 years) with severe traumatic (TBI, N = 20) and non-traumatic (N = 21) brain injuries were studied. Cerebral blood flow velocity, arterial blood pressure and intracranial pressure were repeatedly recorded during 1-h periods. Calculated PRx and Mx were correlated with 3-month clinical outcome score of modified Rankin Scale (mRS) in different subgroups with specific clinical characteristics. Both PRx and Mx correlated significantly with outcome (PRx: r = 0.38, p < 0.05; AUC = 0.64, n.s./Mx: r = 0.48, p < 0.005; AUC = 0.80, p < 0.005) in the overall group, and in patients with hemicraniectomy (N = 17; PRx: r = 0.73, p < 0.001; AUC = 0.89, p < 0.01/Mx: r = 0.69, p < 0.005; AUC = 0.87, p < 0.05). Mx, not PRx, correlated significantly with mRS in patients with heart failure (N = 17; r = 0.69, p < 0.005; AUC = 0.92, p < 0.005), and in non-traumatic patients (r = 0.49, p < 0.05; AUC = 0.79, p < 0.05). PRx, not Mx, correlated significantly with mRS in TBI patients (r = 0.63, p < 0.01; AUC = 0.89, p < 0.01). Both indexes did not correlate with mRS in diabetes patients (N = 15), PRx failed in hypocapnic patients (N = 26). Both PRx and Mx were significantly associated with 3-month clinical outcome, even in patients with hemicraniectomy. PRx was more appropriate for TBI patients, while Mx was better suited for non-traumatic patients and patients with heart failure. Prognostic values of indexes were affected by diabetes (both Mx and PRx) and hypocapnia (PRx only).
Keywords: Cerebral autoregulation; Cerebral blood flow; Cerebrovascular pressure reactivity; Modified Rankin Scale; Stroke; Traumatic brain injury.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
