

Update on Vaccine-Derived Polioviruses - Worldwide, January 2014-March 2015
- PMID: 26086635
- PMCID: PMC4584736
Update on Vaccine-Derived Polioviruses - Worldwide, January 2014-March 2015
Abstract
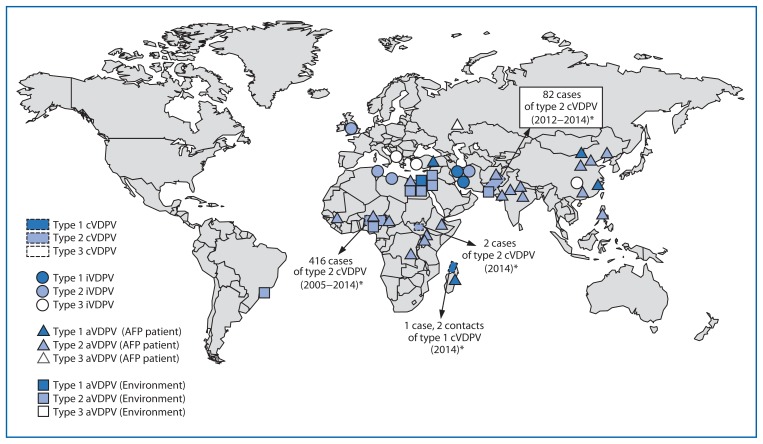
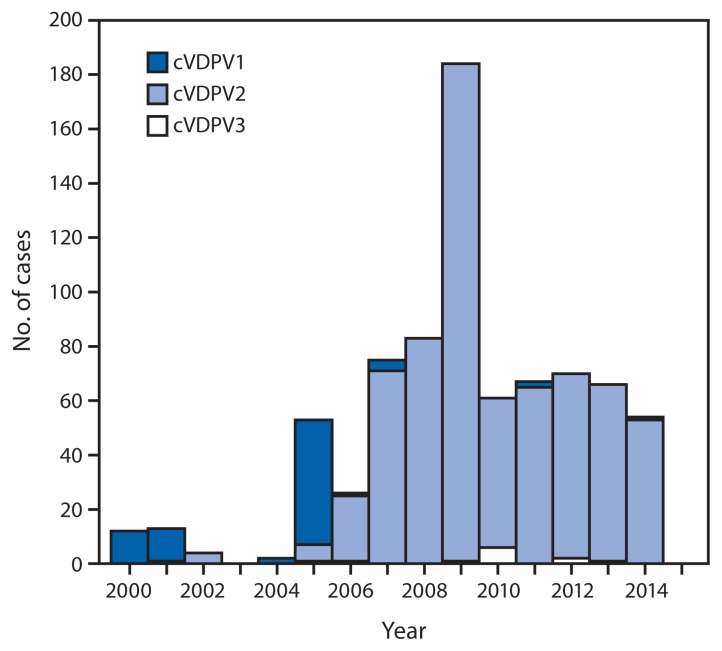
Since the World Health Assembly's 1988 resolution to eradicate poliomyelitis, one of the main tools of the World Health Organization (WHO) Global Polio Eradication Initiative (GPEI) has been the live, attenuated oral poliovirus vaccine (OPV). OPV might require several doses to induce immunity but provides long-term protection against paralytic disease. Through effective use of OPV, GPEI has brought polio to the threshold of eradication. Wild poliovirus type 2 (WPV2) was eliminated in 1999, WPV3 has not been detected since November 2012, and WPV1 circulation appears to be restricted to parts of Pakistan and Afghanistan. However, continued use of OPV carries two key risks. The first, vaccine-associated paralytic poliomyelitis (VAPP) has been recognized since the early 1960s. VAPP is a very rare event that occurs sporadically when an administered dose of OPV reverts to neurovirulence and causes paralysis in the vaccine recipient or a nonimmune contact. VAPP can occur among immunologically normal vaccine recipients and their contacts as well as among persons who have primary immunodeficiencies (PIDs) manifested by defects in antibody production; it is not associated with outbreaks. The second, the emergence of genetically divergent, neurovirulent vaccine-derived polioviruses (VDPVs) was recognized more recently. Circulating VDPVs (cVDPVs) resemble WPVs and, in areas with low OPV coverage, can cause polio outbreaks. Immunodeficiency-associated VDPVs (iVDPVs) can replicate and be excreted for years in some persons with PIDs; GPEI maintains a registry of iVDPV cases. Ambiguous VDPVs (aVDPVs) are isolates that cannot be classified definitively. This report updates previous surveillance summaries and describes VDPVs detected worldwide during January 2014-March 2015. Those include new cVDPV outbreaks in Madagascar and South Sudan, and sharply reduced type 2 cVDPV (cVDPV2) circulation in Nigeria and Pakistan during the latter half of 2014. Eight newly identified persons in six countries were found to excrete iVDPVs, and a patient in the United Kingdom was still excreting iVDPV2 in 2014 after more than 28 years. Ambiguous VDPVs were found among immunocompetent persons and environmental samples in 16 countries. Because the large majority of VDPV case-isolates are type 2, WHO has developed a plan for coordinated worldwide withdrawal of trivalent (types 1, 2, and 3) OPV (tOPV) and replacement with bivalent (types 1 and 3) OPV (bOPV) in April 2016, preceded by introduction of at least 1 dose of injectable inactivated poliovirus vaccine (IPV) into routine immunization schedules worldwide to maintain immunity to type 2 viruses.
Figures
References
-
- Sutter RW, Kew OM, Cochi SL, Aylward RB. Poliovirus vaccine—live. In: Plotkin SA, Orenstein WA, Offit PA, editors. Vaccines. Sixth ed. London, England: W.B. Saunders; 2013. pp. 598–645.
-
- Burns CC, Diop OM, Sutter RW, Kew OM. Vaccine-derived polioviruses. J Infect Dis. 2014;210(Suppl 1):S283–93. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
