

Value of Lung Ultrasonography in the Diagnosis and Outcome Prediction of Pediatric Community-Acquired Pneumonia with Necrotizing Change
- PMID: 26086718
- PMCID: PMC4472812
- DOI: 10.1371/journal.pone.0130082
Value of Lung Ultrasonography in the Diagnosis and Outcome Prediction of Pediatric Community-Acquired Pneumonia with Necrotizing Change
Abstract
Background: Lung ultrasonography has been advocated in diagnosing pediatric community-acquired pneumonia. However, its function in identifying necrotizing pneumonia, a complication, has not been explored. This study investigated the value of lung ultrasonography in diagnosing pediatric necrotizing pneumonia and its role in predicting clinical outcomes.
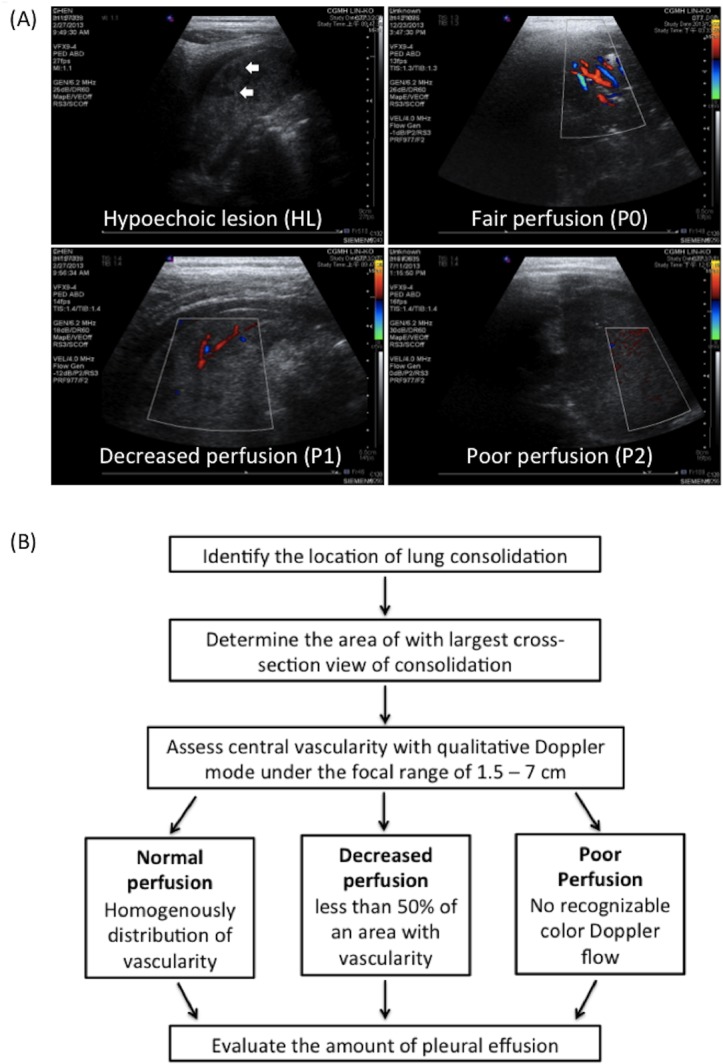
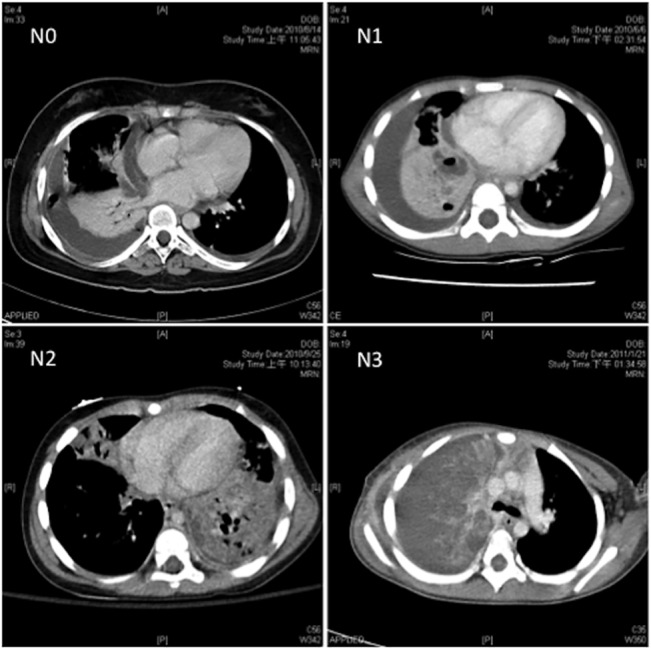
Methods: We retrospectively reviewed 236 children with community-acquired pneumonia who were evaluated using lung ultrasonography within 2-3 days after admission. The ultrasonographic features assessed included lung perfusion, the presence of hypoechoic lesions, and the amount of pleural effusion. Chest computed tomography was also performed in 96 patients as clinically indicated. Detailed records of clinical information were obtained.
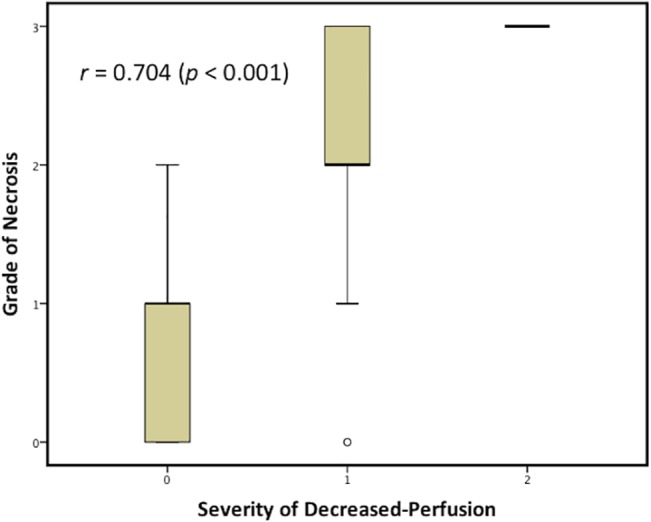
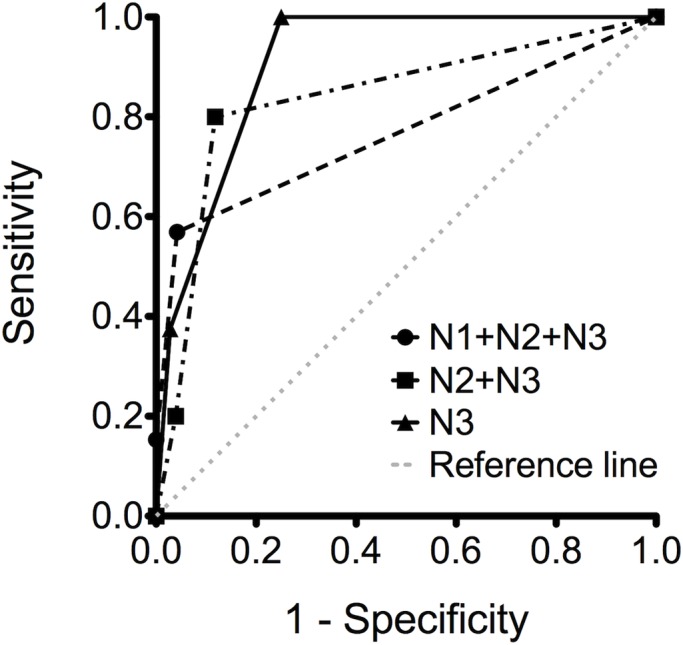
Results: Our results showed a high correlation between the degree of impaired perfusion in ultrasonography and the severity of necrosis in computed tomography (r = 0.704). The degree of impaired perfusion can favorably be used to predict massive necrosis in computed tomography (area under the receiver operating characteristic curve, 0.908). The characteristics of impaired perfusion and hypoechoic lesions in ultrasonography were associated with an increased risk of pneumatocele formation (odds ratio (OR), 10.11; 95% CI, 2.95-34.64) and the subsequent requirement for surgical lung resection (OR, 8.28; 95% CI, 1.86-36.93). Furthermore, a longer hospital stay would be expected if moderate-to-massive pleural effusion was observed in addition to impaired perfusion in ultrasonography (OR, 3.08; 95% CI, 1.15-8.29).
Conclusion: Lung ultrasonography is favorably correlated with chest computed tomography in the diagnosis of necrotizing pneumonia, especially regarding massive necrosis of the lung. Because it is a simple and reliable imaging tool that is valuable in predicting clinical outcomes, we suggest that ultrasonography be applied as a surrogate for computed tomography for the early detection of severe necrotizing pneumonia in children.
Conflict of interest statement
Figures
References
-
- McCarthy VP, Patamasucon P, Gaines T, Lucas MA. Necrotizing pneumococcal pneumonia in childhood. Pediatr Pulmonol. 1999;28: 217–221. - PubMed
-
- Hsieh YC, Hsueh PR, Chun Yi L, Lee PI, Lee CY, Huang LM. Clinical manifestations and molecular epidemiology of necrotizing pneumonia and empyema caused by Streptococcus pneumoniae in children in Taiwan. Clin Infect Dis. 2004;38: 830–835. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
