

The Pathogenesis and Management of Achalasia: Current Status and Future Directions
- PMID: 26087861
- PMCID: PMC4477988
- DOI: 10.5009/gnl14446
The Pathogenesis and Management of Achalasia: Current Status and Future Directions
Abstract
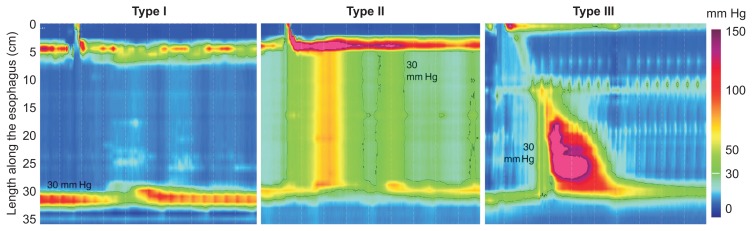
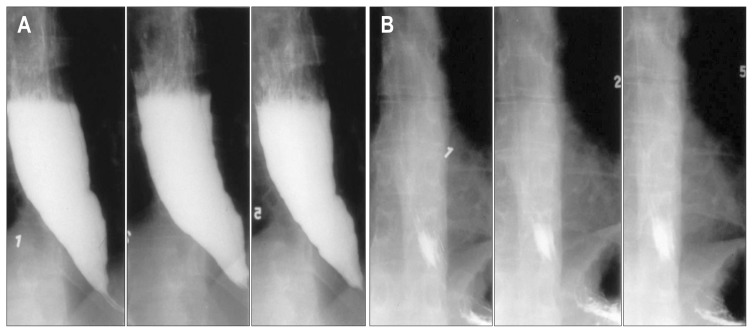
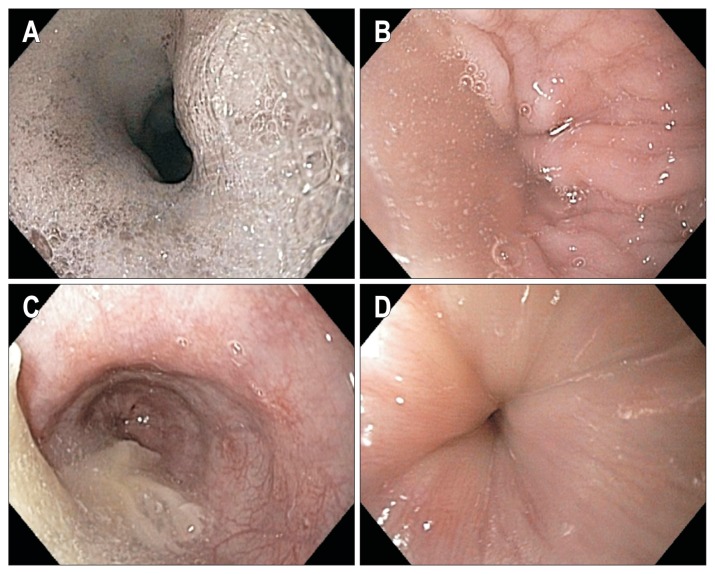
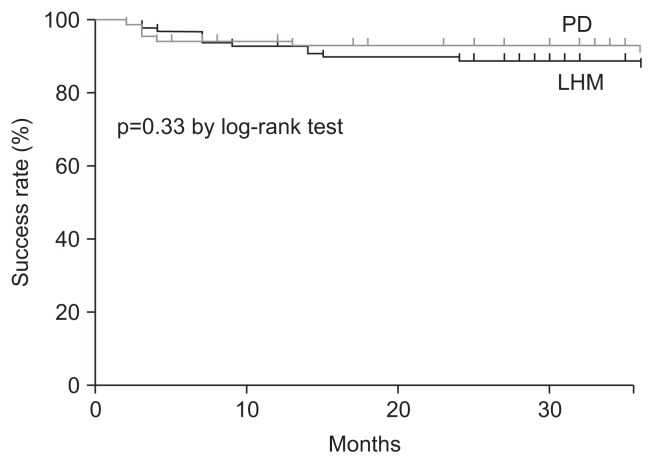
Achalasia is an esophageal motility disorder that is commonly misdiagnosed initially as gastroesophageal reflux disease. Patients with achalasia often complain of dysphagia with solids and liquids but may focus on regurgitation as the primary symptom, leading to initial misdiagnosis. Diagnostic tests for achalasia include esophageal motility testing, esophagogastroduodenoscopy and barium swallow. These tests play a complimentary role in establishing the diagnosis of suspected achalasia. High-resolution manometry has now identified three subtypes of achalasia, with therapeutic implications. Pneumatic dilation and surgical myotomy are the only definitive treatment options for patients with achalasia who can undergo surgery. Botulinum toxin injection into the lower esophageal sphincter should be reserved for those who cannot undergo definitive therapy. Close follow-up is paramount because many patients will have a recurrence of symptoms and require repeat treatment.
Keywords: Peroral esophageal myotomy; Pneumatic dilation; Surgical myotomy.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
