

Symptom recovery after thoracic surgery: Measuring patient-reported outcomes with the MD Anderson Symptom Inventory
- PMID: 26088408
- PMCID: PMC4554973
- DOI: 10.1016/j.jtcvs.2015.05.057
Symptom recovery after thoracic surgery: Measuring patient-reported outcomes with the MD Anderson Symptom Inventory
Abstract
Objectives: Measuring patient-reported outcomes (PROs) has become increasingly important for assessing quality of care and guiding patient management. However, PROs have yet to be integrated with traditional clinical outcomes (such as length of hospital stay), to evaluate perioperative care. This study aimed to use longitudinal PRO assessments to define the postoperative symptom recovery trajectory in patients undergoing thoracic surgery for lung cancer.
Methods: Newly diagnosed patients (N = 60) with stage I or II non-small cell lung cancer who underwent either standard open thoracotomy or video-assisted thoracoscopic surgery lobectomy reported multiple symptoms from before surgery to 3 months after surgery, using the MD Anderson Symptom Inventory. We conducted Kaplan-Meier analyses to determine when symptoms returned to presurgical levels and to mild-severity levels during recovery.
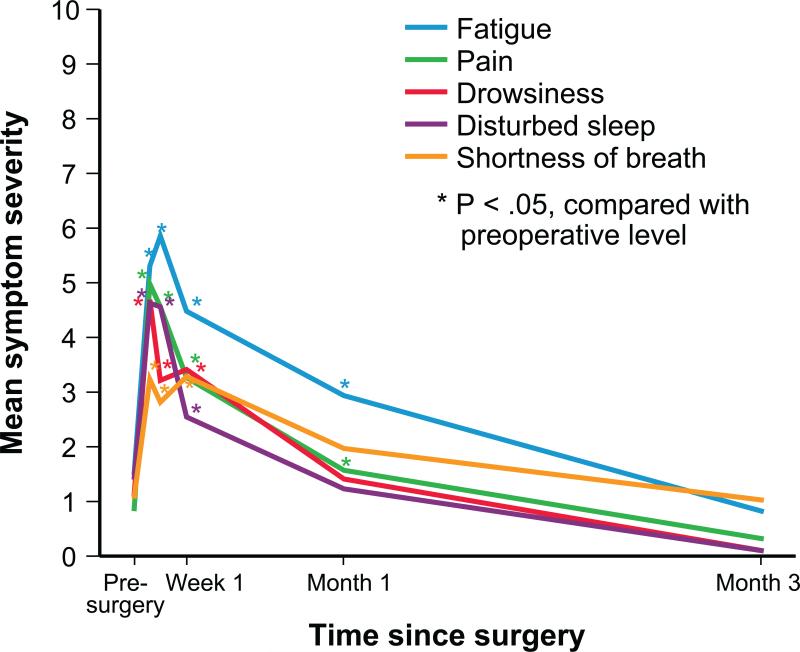
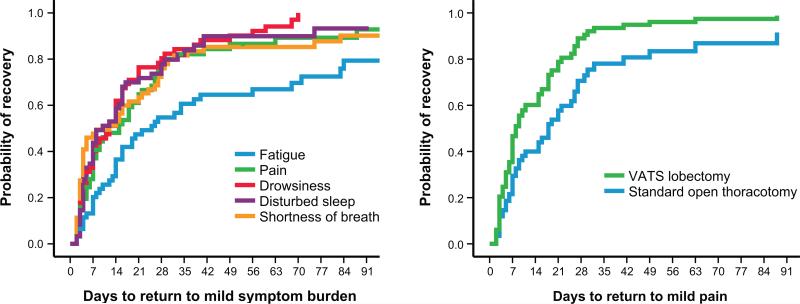
Results: The most-severe postoperative symptoms were fatigue, pain, shortness of breath, disturbed sleep, and drowsiness. The median time to return to mild symptom severity for these 5 symptoms was shorter than the time to return to baseline severity, with fatigue taking longer. Recovery from pain occurred more quickly for patients who underwent lobectomy versus thoracotomy (8 vs 18 days, respectively; P = .022). Patients who had poor preoperative performance status or comorbidities reported higher postoperative pain (all P < .05).
Conclusions: Assessing symptoms from the patient's perspective throughout the postoperative recovery period is an effective strategy for evaluating perioperative care. This study demonstrates that the MD Anderson Symptom Inventory is a sensitive tool for detecting symptomatic recovery, with an expected relationship among surgery type, preoperative performance status, and comorbid conditions.
Keywords: MDASI; VATS; enhanced recovery; patient-reported outcome (PRO); postoperative care; symptoms.
Copyright © 2015 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Measuring postoperative patient outcomes: Who knows best?J Thorac Cardiovasc Surg. 2015 Sep;150(3):619-20. doi: 10.1016/j.jtcvs.2015.06.017. Epub 2015 Jun 14. J Thorac Cardiovasc Surg. 2015. PMID: 26149099 No abstract available.
-
Patient-reported outcomes and importance of their appropriate statistical analyses.J Thorac Cardiovasc Surg. 2015 Sep;150(3):461-2. doi: 10.1016/j.jtcvs.2015.07.043. Epub 2015 Jul 18. J Thorac Cardiovasc Surg. 2015. PMID: 26319459 No abstract available.
References
-
- Ghaferi AA, Birkmeyer JD, Dimick JB. Variation in hospital mortality associated with inpatient surgery. N Engl J Med. 2009;361:1368–75. - PubMed
-
- Aloia TA, Lee JE, Vauthey JN, Abdalla EK, Wolff RA, Varadhachary GR, et al. Delayed recovery after pancreaticoduodenectomy: a major factor impairing the delivery of adjuvant therapy? J Am Coll Surg. 2007;204:347–55. - PubMed
-
- Kehlet H, Mythen M. Why is the surgical high-risk patient still at risk? Br J Anaesth. 2011;106:289–91. - PubMed
-
- Varadhan KK, Neal KR, Dejong CH, Fearon KC, Ljungqvist O, Lobo DN. The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr. 2010;29:434–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
