

From Learning to Memory: What Flies Can Tell Us about Intellectual Disability Treatment
- PMID: 26089803
- PMCID: PMC4453272
- DOI: 10.3389/fpsyt.2015.00085
From Learning to Memory: What Flies Can Tell Us about Intellectual Disability Treatment
Abstract
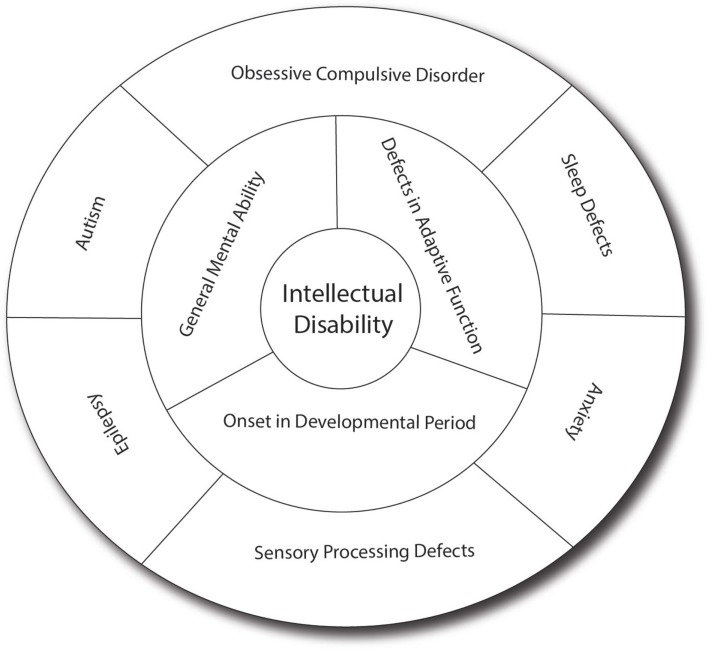
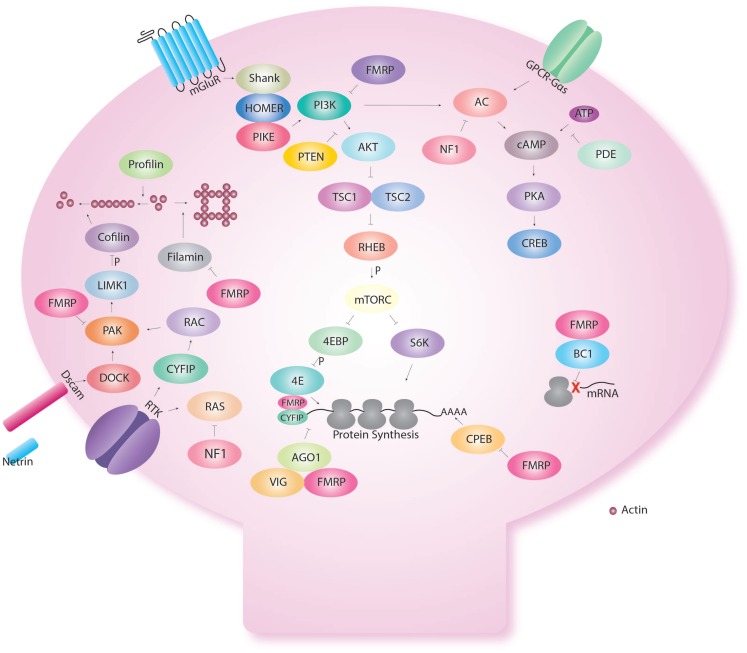
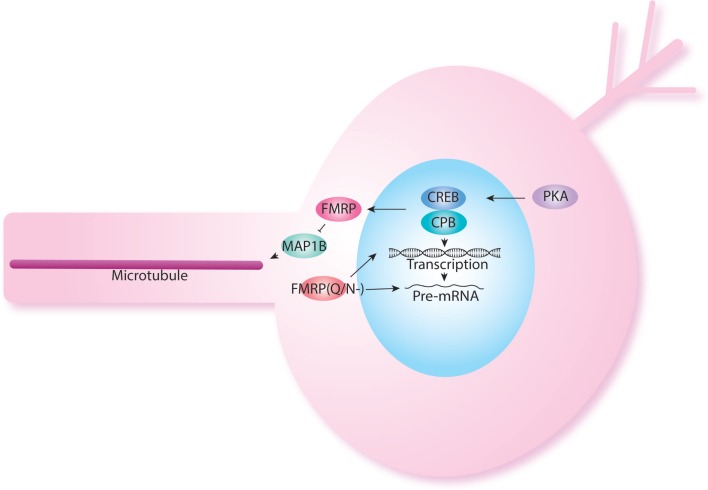
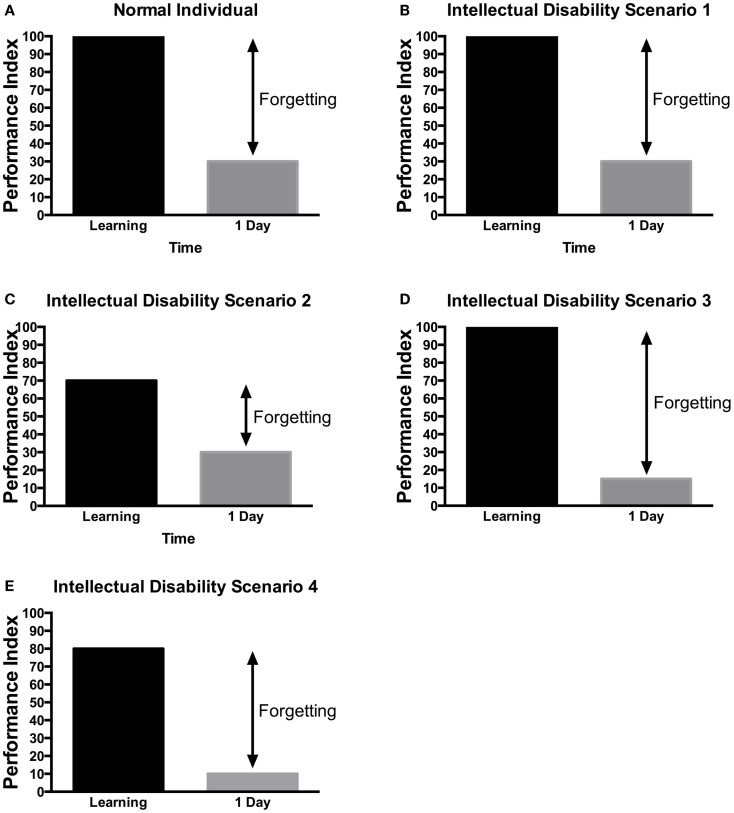
Intellectual disability (ID), previously known as mental retardation, affects 3% of the population and remains without pharmacological treatment. ID is characterized by impaired general mental abilities associated with defects in adaptive function in which onset occurs before 18 years of age. Genetic factors are increasing and being recognized as the causes of severe ID due to increased use of genome-wide screening tools. Unfortunately drug discovery for treatment of ID has not followed the same pace as gene discovery, leaving clinicians, patients, and families without the ability to ameliorate symptoms. Despite this, several model organisms have proven valuable in developing and screening candidate drugs. One such model organism is the fruit fly Drosophila. First, we review the current understanding of memory in human and its model in Drosophila. Second, we describe key signaling pathways involved in ID and memory such as the cyclic adenosine 3',5'-monophosphate (cAMP)-cAMP response element binding protein (CREB) pathway, the regulation of protein synthesis, the role of receptors and anchoring proteins, the role of neuronal proliferation, and finally the role of neurotransmitters. Third, we characterize the types of memory defects found in patients with ID. Finally, we discuss how important insights gained from Drosophila learning and memory could be translated in clinical research to lead to better treatment development.
Keywords: Drosophila; clinical trials; fragile X; intellectual disability; learning; memory.
Figures
References
-
- Svenaeus F. Diagnostic and statistical manual of mental disorders, 5th edition. Med Health Care Philos (2014) 17:241–4.10.1007/s11019-013-9529-6 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases