

International consensus diagnostic criteria for neuromyelitis optica spectrum disorders
- PMID: 26092914
- PMCID: PMC4515040
- DOI: 10.1212/WNL.0000000000001729
International consensus diagnostic criteria for neuromyelitis optica spectrum disorders
Abstract
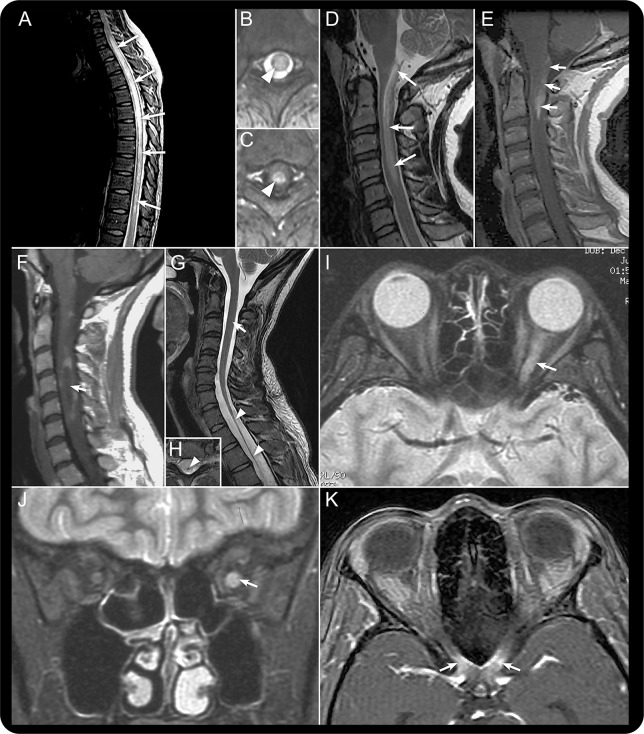
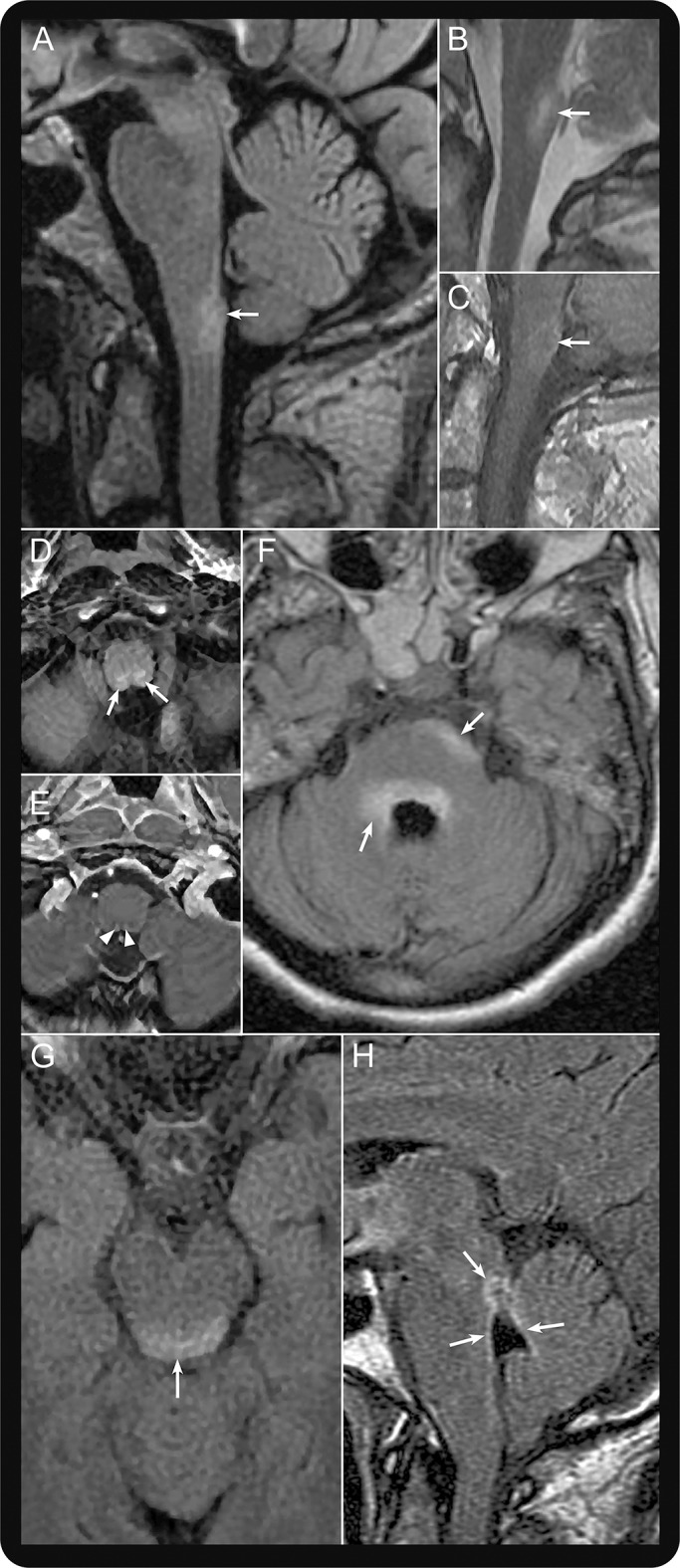
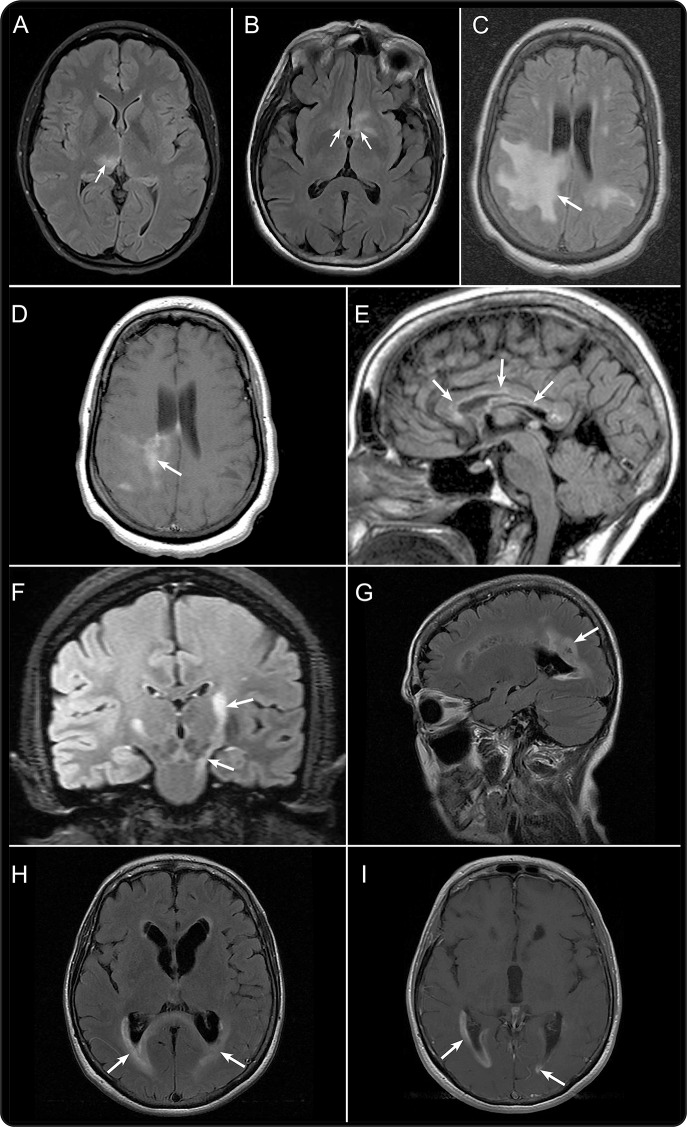
Neuromyelitis optica (NMO) is an inflammatory CNS syndrome distinct from multiple sclerosis (MS) that is associated with serum aquaporin-4 immunoglobulin G antibodies (AQP4-IgG). Prior NMO diagnostic criteria required optic nerve and spinal cord involvement but more restricted or more extensive CNS involvement may occur. The International Panel for NMO Diagnosis (IPND) was convened to develop revised diagnostic criteria using systematic literature reviews and electronic surveys to facilitate consensus. The new nomenclature defines the unifying term NMO spectrum disorders (NMOSD), which is stratified further by serologic testing (NMOSD with or without AQP4-IgG). The core clinical characteristics required for patients with NMOSD with AQP4-IgG include clinical syndromes or MRI findings related to optic nerve, spinal cord, area postrema, other brainstem, diencephalic, or cerebral presentations. More stringent clinical criteria, with additional neuroimaging findings, are required for diagnosis of NMOSD without AQP4-IgG or when serologic testing is unavailable. The IPND also proposed validation strategies and achieved consensus on pediatric NMOSD diagnosis and the concepts of monophasic NMOSD and opticospinal MS.
© 2015 American Academy of Neurology.
Figures
Comment in
-
Pushing the boundaries of neuromyelitis optica: does antibody make the disease?Neurology. 2015 Jul 14;85(2):118-9. doi: 10.1212/WNL.0000000000001749. Epub 2015 Jun 19. Neurology. 2015. PMID: 26092912 No abstract available.
-
Neuromyelitis optica and neuromyelitis optica like spectrum disorders: Is it not the time to change the criteria?Mult Scler Relat Disord. 2018 Feb;20:153. doi: 10.1016/j.msard.2018.01.022. Epub 2018 Mar 20. Mult Scler Relat Disord. 2018. PMID: 29414289 No abstract available.
References
-
- Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica. Lancet Neurol 2007;6:805–815. - PubMed
-
- Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006;66:1485–1489. - PubMed
-
- Wingerchuk DM, Hogancamp WF, O'Brien PC, Weinshenker BG. The clinical course of neuromyelitis optica (Devic's syndrome). Neurology 1999;53:1107–1114. - PubMed
-
- Lennon VA, Wingerchuk DM, Kryzer TJ, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet 2004;364:2106–2112. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical