

Increased speed and image quality in single-shot fast spin echo imaging via variable refocusing flip angles
- PMID: 26094580
- PMCID: PMC4684814
- DOI: 10.1002/jmri.24941
Increased speed and image quality in single-shot fast spin echo imaging via variable refocusing flip angles
Abstract
Purpose: To develop and validate clinically a single-shot fast spin echo (SSFSE) sequence utilizing variable flip angle refocusing pulses to shorten acquisition times via reductions in specific absorption rate (SAR) and improve image quality.
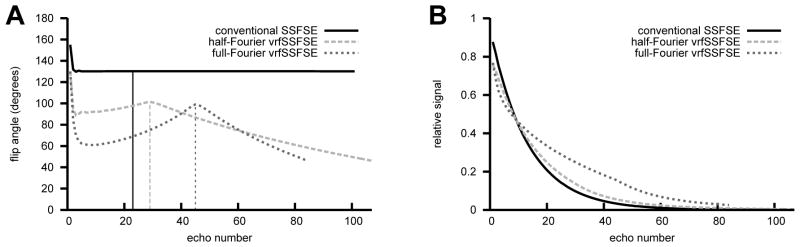
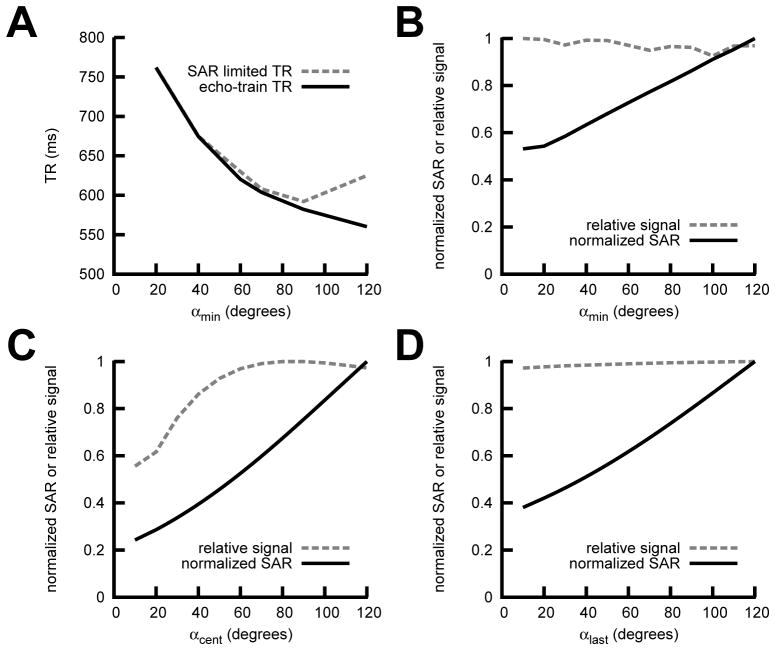
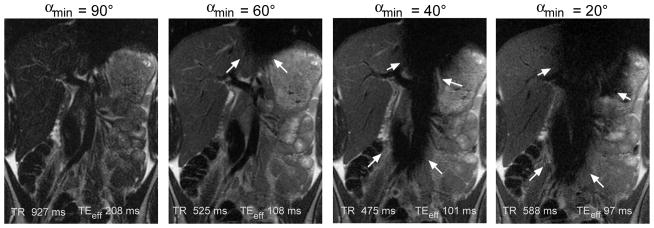
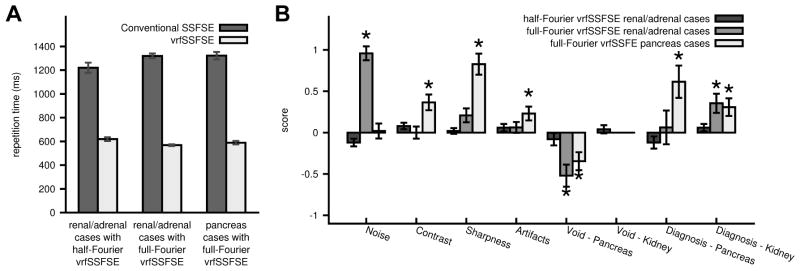
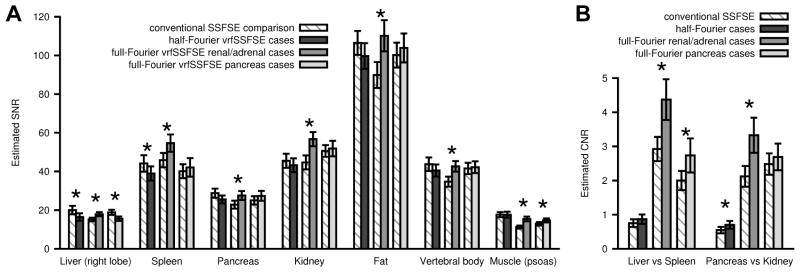
Materials and methods: A variable refocusing flip angle SSFSE sequence (vrfSSFSE) was designed and implemented, with simulations and volunteer scans performed to determine suitable flip angle modulation parameters. With Institutional Review Board (IRB) approval/informed consent, patients referred for 3T abdominal magnetic resonance imaging (MRI) were scanned with conventional SSFSE and either half-Fourier (n = 25) or full-Fourier vrfSSFSE (n = 50). Two blinded radiologists semiquantitatively scored images on a scale from -2 to 2 for contrast, noise, sharpness, artifacts, cardiac motion-related signal loss, and the ability to evaluate the pancreas and kidneys.
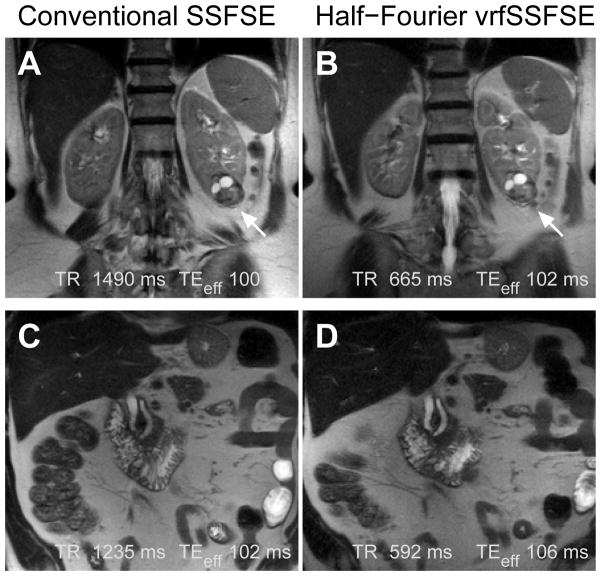
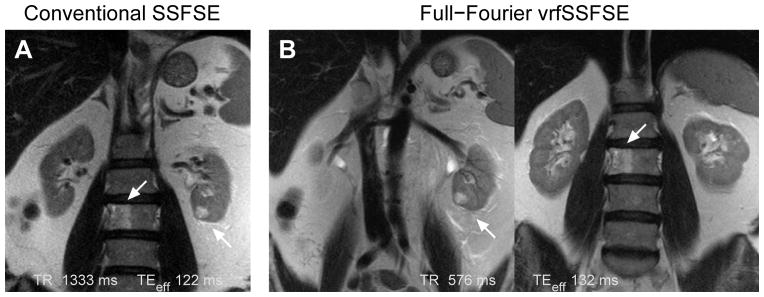
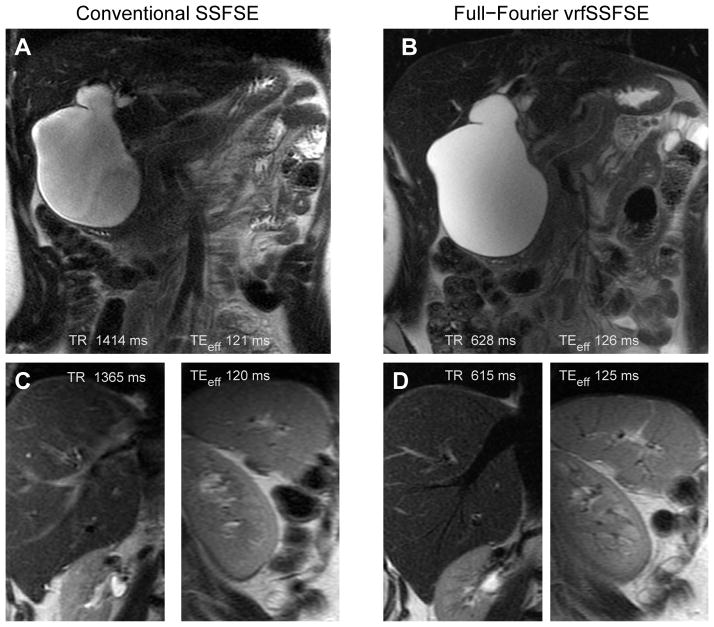
Results: vrfSSFSE demonstrated significantly increased speed (∼2-fold, P < 0.0001). Significant improvements in image quality parameters with full-Fourier vrfSSFSE included increased contrast, sharpness, and visualization of pancreatic and renal structures with higher bandwidth technique (mean scores 0.37, 0.83, 0.62, and 0.31, respectively, P ≤ 0.001), and decreased image noise and improved visualization of renal structures when used with an equal bandwidth technique (mean scores 0.96 and 0.35, respectively, P < 0.001). Increased cardiac motion-related signal loss with full-Fourier vrfSSFSE was seen in the pancreas but not the kidney.
Conclusion: vrfSSFSE increases speed at 3T over conventional SSFSE via reduced SAR, and when combined with full-Fourier acquisition can improve image quality, although with some increased sensitivity to cardiac motion-related signal loss.
Keywords: echo stabilization; single shot fast spin echo; specific absorption rate; variable refocusing flip angle.
© 2015 Wiley Periodicals, Inc.
Figures
References
-
- Chavhan GB, Babyn PS, Vasanawala SS. Abdominal MR imaging in children: motion compensation, sequence optimization, and protocol organization. Radiographics. 2013;33:703–719. - PubMed
-
- Yang RK, Roth CG, Ward RJ, deJesus JO, Mitchell DG. Optimizing abdominal MR imaging: approaches to common problems. Radiographics. 2010:185–199. - PubMed
-
- Bhosale P, Ma J, Choi H. Utility of the FIESTA pulse sequence in body oncologic imaging: review. AJR Am J Roentgenol. 2009;192:S83–93. - PubMed
-
- Hennig J, Weigel M, Scheffler K. Multiecho sequences with variable refocusing flip angles: optimization of signal behavior using smooth transitions between pseudo steady states (TRAPS) Magn Reson Med. 2003;49:527–535. - PubMed
-
- Madhuranthakam AJ, Busse RF, Brittain JH, Rofsky NM, Alsop DC. Sensitivity of low flip angle SSFSE of the abdomen to cardiac motion. Proceedings of the 15th Annual Meeting of ISMRM; Berlin, Germany. 2007; p. abstract 2523.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
