

Sitagliptin improves glycaemic excursion after a meal or after an oral glucose load in Japanese subjects with impaired glucose tolerance
- PMID: 26094974
- PMCID: PMC5034821
- DOI: 10.1111/dom.12507
Sitagliptin improves glycaemic excursion after a meal or after an oral glucose load in Japanese subjects with impaired glucose tolerance
Abstract
Aims: To evaluate the efficacy and tolerability of sitagliptin in subjects with impaired glucose tolerance (IGT).
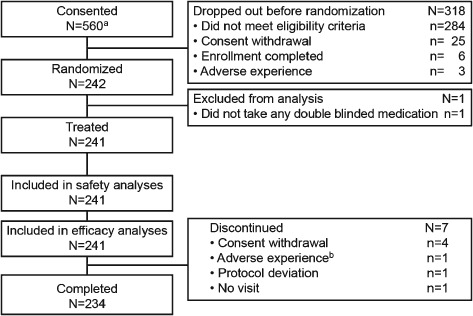
Methods: In a double-blind, parallel-group study, 242 Japanese subjects with IGT, determined by a 75-g oral glucose tolerance test (OGTT) at week -1, were randomized (1 : 1 : 1) to placebo (n = 83), sitagliptin 25 mg (n = 82) or 50 mg (n = 77) once daily for 8 weeks. Glycaemic variables were assessed using another OGTT at week 7 and meal tolerance tests (MTTs) at weeks 0 and 8. Primary and secondary endpoints were percent change from baseline in glucose total area under the curve 0-2 h (AUC(0 -2 h)) during the MTT and OGTT, respectively.
Results: Least squares mean percent change from baseline in glucose AUC(0 -2 h) during the MTT were -2.4, -9.5 and -11.5%, and during the OGTT were -3.7, -21.4 and -20.1% with placebo, sitagliptin 25 mg once daily, and 50 mg once daily, respectively (p < 0.001 for either sitagliptin dose vs placebo in both tests). Sitagliptin treatment enhanced early insulin response during the OGTT and decreased total insulin response, assessed as the total AUC(0 -2 h) during the MTT. Sitagliptin treatment also suppressed glucagon response during the MTT. The incidence of adverse events, including hypoglycaemia, was low and generally similar in all treatment groups.
Conclusions: Treatment with sitagliptin significantly reduced glucose excursions during both an MTT and an OGTT; this effect was associated with an increase in early insulin secretion after oral glucose loading as well as a blunted glucagon response during an MTT. Sitagliptin was generally well tolerated in subjects with IGT.
Trial registration: ClinicalTrials.gov NCT01405911.
Keywords: DPP-4; MK-0431; dipeptidyl peptidase-4 inhibitors; incretins.
© 2015 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Figures
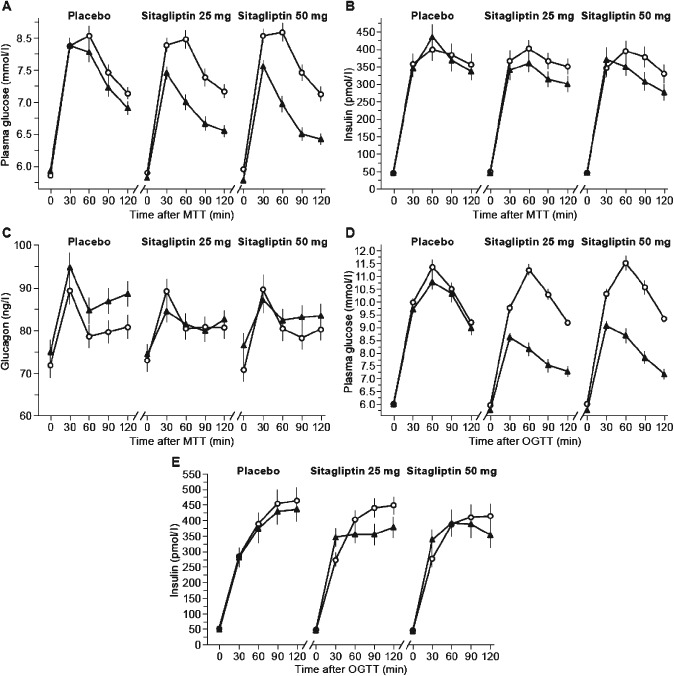
 ) and at week 8 of treatment (
) and at week 8 of treatment ( ) and on glucose (D) and insulin (E) during oral glucose tolerance test (
) and on glucose (D) and insulin (E) during oral glucose tolerance test ( ) and at week 7 of treatment (
) and at week 7 of treatment ( ). Data shown are mean ± standard error.
). Data shown are mean ± standard error.References
-
- Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 1997; 20: 1183–1197. - PubMed
-
- Glucose tolerance and cardiovascular mortality: comparison of fasting and 2‐hour diagnostic criteria. Arch Intern Med 2001; 161: 397–405. - PubMed
-
- Nakagami T; DECODA Study Group . Hyperglycaemia and mortality from all causes and from cardiovascular disease in five populations of Asian origin. Diabetologia 2004; 47:385–394. - PubMed
-
- Tominaga M, Eguchi H, Manaka H, Igarashi K, Kato T, Sekikawa A. Impaired glucose tolerance is a risk factor for cardiovascular disease, but not impaired fasting glucose. The Funagata diabetes study. Diabetes Care 1999; 22: 920–924. - PubMed
-
- Kahn SE, Haffner SM, Heise MA et al. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med 2006; 355: 2427–2443. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
