

Facilitators and Barriers to Safe Medication Administration to Hospital Inpatients: A Mixed Methods Study of Nurses' Medication Administration Processes and Systems (the MAPS Study)
- PMID: 26098106
- PMCID: PMC4476704
- DOI: 10.1371/journal.pone.0128958
Facilitators and Barriers to Safe Medication Administration to Hospital Inpatients: A Mixed Methods Study of Nurses' Medication Administration Processes and Systems (the MAPS Study)
Abstract
Context: Research has documented the problem of medication administration errors and their causes. However, little is known about how nurses administer medications safely or how existing systems facilitate or hinder medication administration; this represents a missed opportunity for implementation of practical, effective, and low-cost strategies to increase safety.
Aim: To identify system factors that facilitate and/or hinder successful medication administration focused on three inter-related areas: nurse practices and workarounds, workflow, and interruptions and distractions.
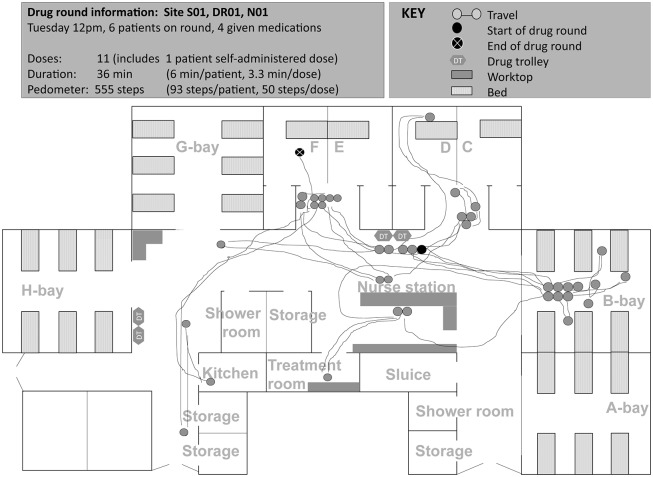
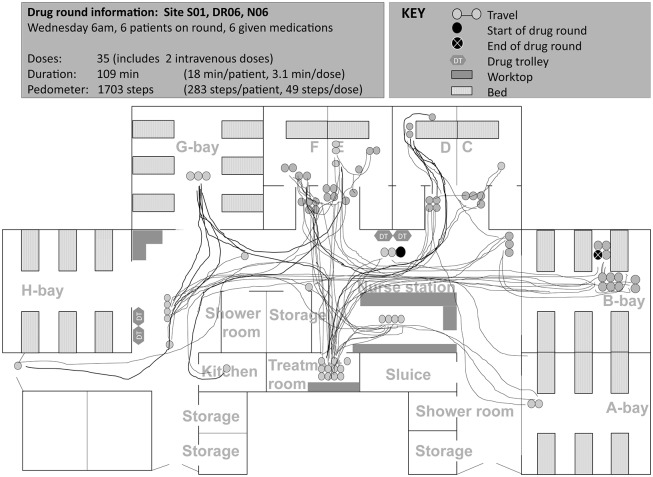
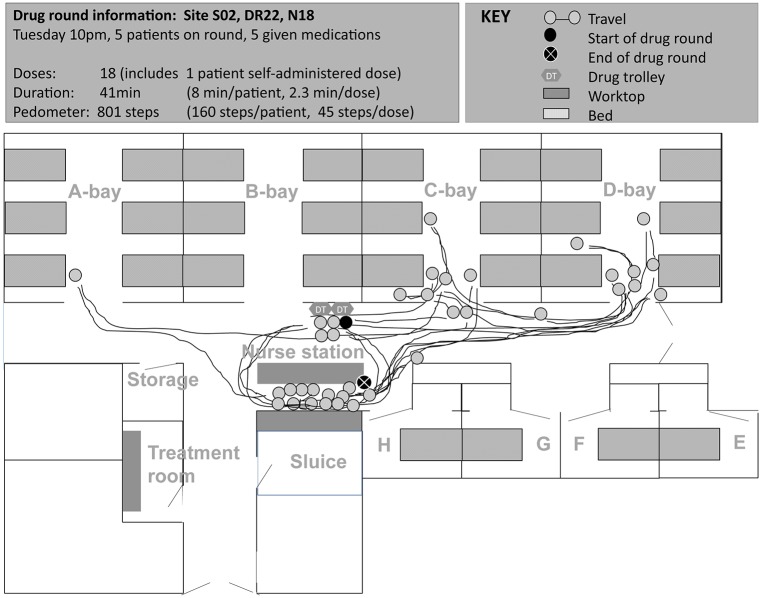
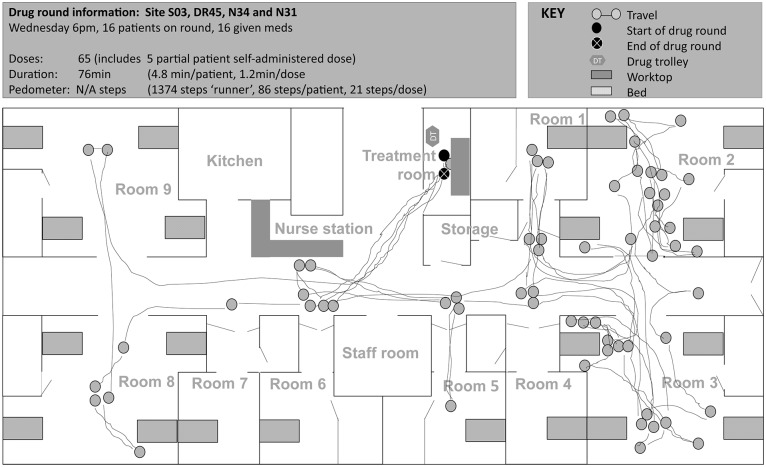
Methods: We used a mixed-methods ethnographic approach involving observational fieldwork, field notes, participant narratives, photographs, and spaghetti diagrams to identify system factors that facilitate and/or hinder successful medication administration in three inpatient wards, each from a different English NHS trust. We supplemented this with quantitative data on interruptions and distractions among other established medication safety measures.
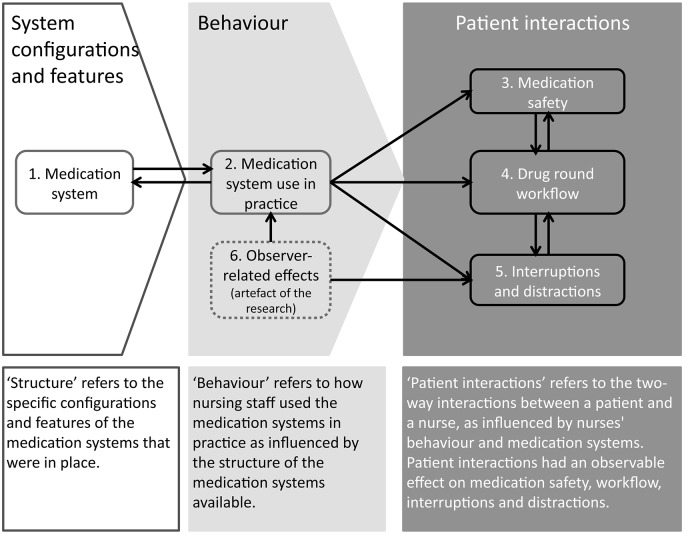
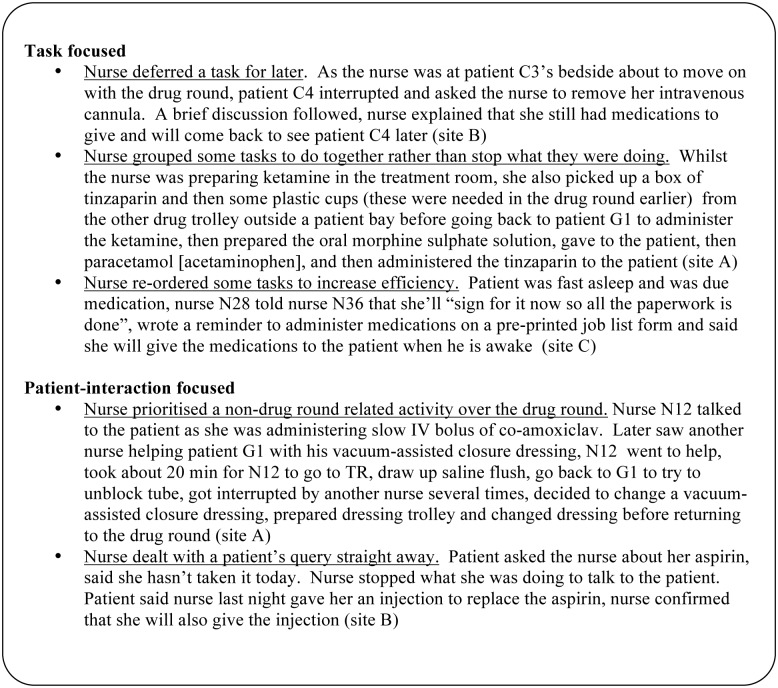
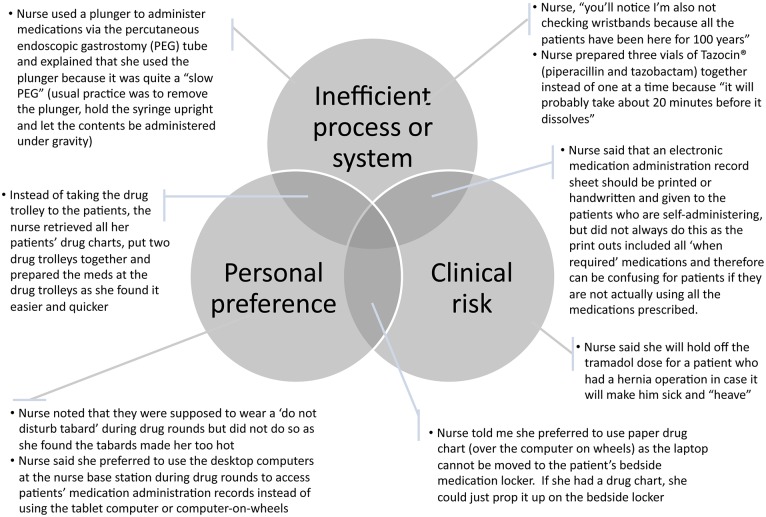
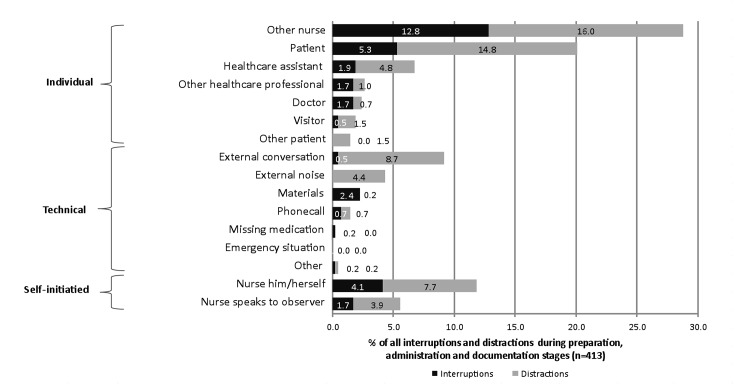
Findings: Overall, 43 nurses on 56 drug rounds were observed. We identified a median of 5.5 interruptions and 9.6 distractions per hour. We identified three interlinked themes that facilitated successful medication administration in some situations but which also acted as barriers in others: (1) system configurations and features, (2) behaviour types among nurses, and (3) patient interactions. Some system configurations and features acted as a physical constraint for parts of the drug round, however some system effects were partly dependent on nurses' inherent behaviour; we grouped these behaviours into 'task focused', and 'patient-interaction focused'. The former contributed to a more streamlined workflow with fewer interruptions while the latter seemed to empower patients to act as a defence barrier against medication errors by being: (1) an active resource of information, (2) a passive information resource, and/or (3) a 'double-checker'.
Conclusions: We have identified practical examples of system effects on work optimisation and nurse behaviours that potentially increase medication safety, and conceptualized ways in which patient involvement can increase medication safety in hospitals.
Conflict of interest statement
Figures
References
-
- McLeod M. Medication administration processes and systems—exploring the effects of systems-based variation on the safety of medication administration in the UK National Health Service [PhD thesis]. London: University College London, The School of Pharmacy; 2013.
-
- Kohn L, Corrigan J, Donaldson M. To err is human: Building a safer health system. Washington, DC: National Academy Press; 1999. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
